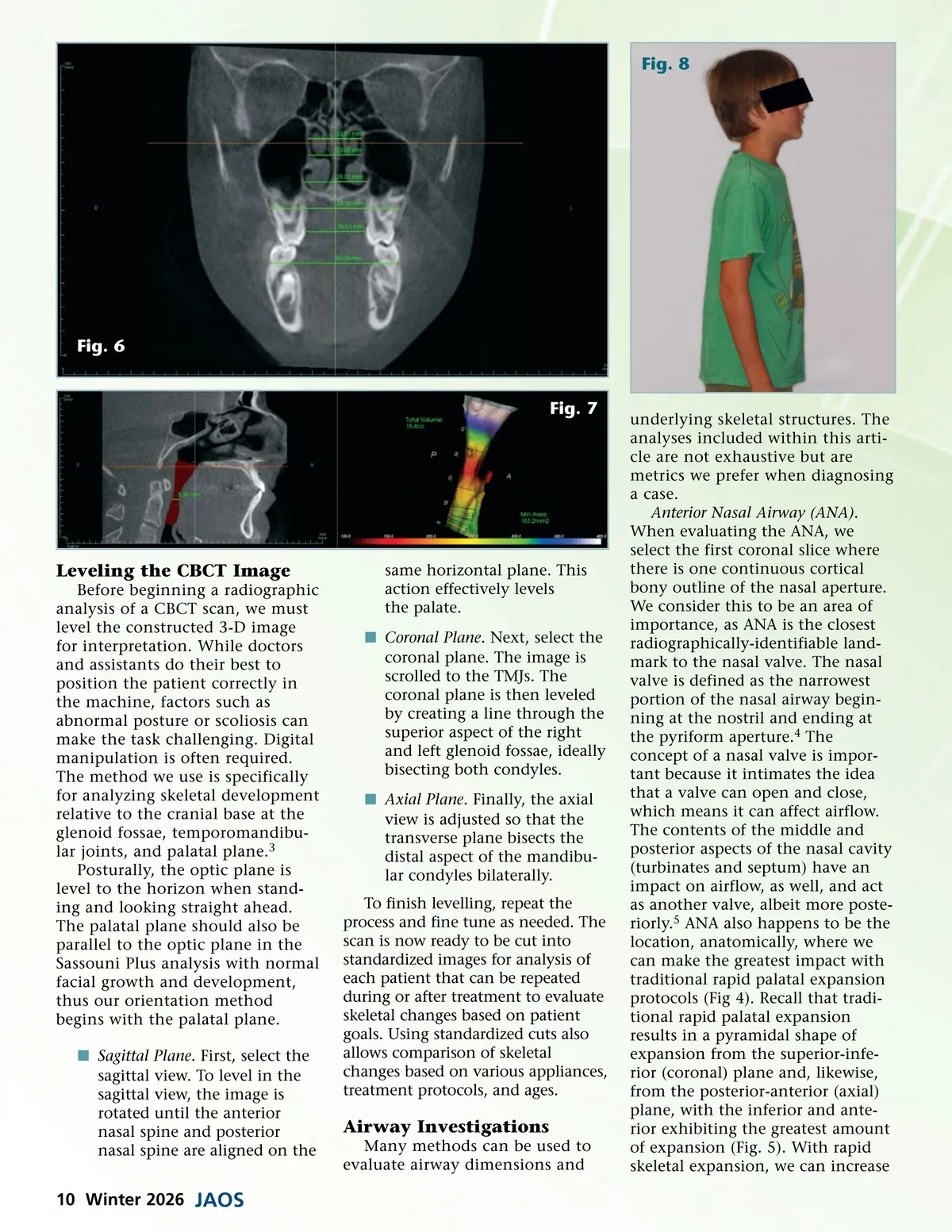
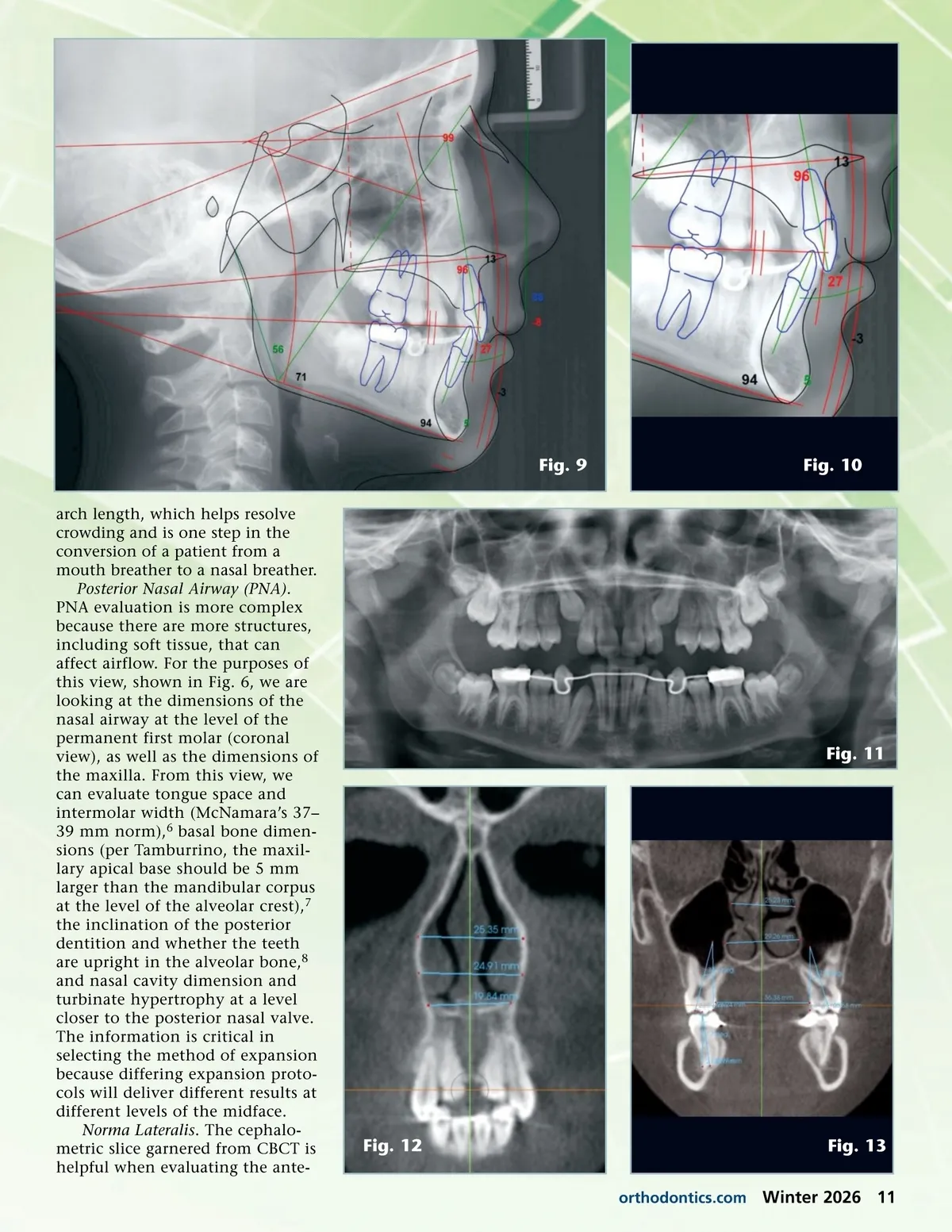
Fig. 9 arch length, which helps resolve crowding and is one step in the conversion of a patient from a mouth breather to a nasal breather. Posterior Nasal Airway (PNA) . PNA evaluation is more complex because there are more structures, including soft tissue, that can affect airflow. For the purposes of this view, shown in Fig. 6, we are looking at the dimensions of the nasal airway at the level of the permanent first molar (coronal view), as well as the dimensions of the maxilla. From this view, we can evaluate tongue space and intermolar width (McNamara’s 37– 39 mm norm), 6 basal bone dimen-sions (per Tamburrino, the maxil-lary apical base should be 5 mm larger than the mandibular corpus at the level of the alveolar crest), 7 the inclination of the posterior dentition and whether the teeth are upright in the alveolar bone, 8 and nasal cavity dimension and turbinate hypertrophy at a level closer to the posterior nasal valve. The information is critical in selecting the method of expansion because differing expansion proto-cols will deliver different results at different levels of the midface. Norma Lateralis . The cephalo-metric slice garnered from CBCT is helpful when evaluating the ante-Fig. 10 Fig. 11 Fig. 12 orthodontics.com Fig. 13 Winter 2026 11
Journal of the American Orthodontic Society Winter 2026: Page 11