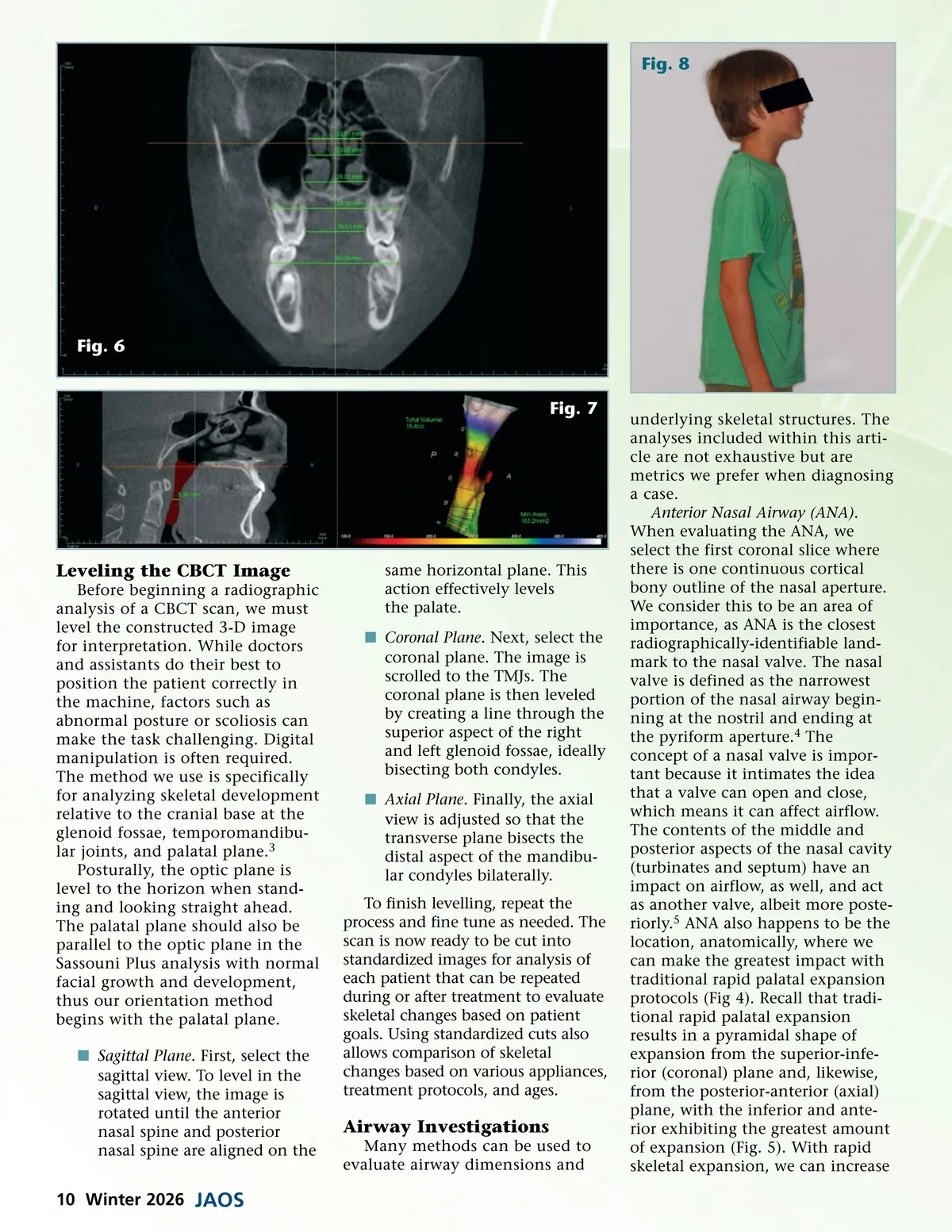
Fig. 8 Fig. 6 Fig. 7 Leveling the CBCT Image Before beginning a radiographic analysis of a CBCT scan, we must level the constructed 3-D image for interpretation. While doctors and assistants do their best to position the patient correctly in the machine, factors such as abnormal posture or scoliosis can make the task challenging. Digital manipulation is often required. The method we use is specifically for analyzing skeletal development relative to the cranial base at the glenoid fossae, temporomandibu-lar joints, and palatal plane. 3 Posturally, the optic plane is level to the horizon when stand-ing and looking straight ahead. The palatal plane should also be parallel to the optic plane in the Sassouni Plus analysis with normal facial growth and development, thus our orientation method begins with the palatal plane. í Sagittal Plane . First, select the sagittal view. To level in the sagittal view, the image is rotated until the anterior nasal spine and posterior nasal spine are aligned on the same horizontal plane. This action effectively levels the palate. í Coronal Plane . Next, select the coronal plane. The image is scrolled to the TMJs. The coronal plane is then leveled by creating a line through the superior aspect of the right and left glenoid fossae, ideally bisecting both condyles. í Axial Plane . Finally, the axial view is adjusted so that the transverse plane bisects the distal aspect of the mandibu-lar condyles bilaterally. To finish levelling, repeat the process and fine tune as needed. The scan is now ready to be cut into standardized images for analysis of each patient that can be repeated during or after treatment to evaluate skeletal changes based on patient goals. Using standardized cuts also allows comparison of skeletal changes based on various appliances, treatment protocols, and ages. Airway Investigations Many methods can be used to evaluate airway dimensions and underlying skeletal structures. The analyses included within this arti-cle are not exhaustive but are metrics we prefer when diagnosing a case. Anterior Nasal Airway (ANA) . When evaluating the ANA, we select the first coronal slice where there is one continuous cortical bony outline of the nasal aperture. We consider this to be an area of importance, as ANA is the closest radiographically-identifiable land-mark to the nasal valve. The nasal valve is defined as the narrowest portion of the nasal airway begin-ning at the nostril and ending at the pyriform aperture. 4 The concept of a nasal valve is impor-tant because it intimates the idea that a valve can open and close, which means it can affect airflow. The contents of the middle and posterior aspects of the nasal cavity (turbinates and septum) have an impact on airflow, as well, and act as another valve, albeit more poste-riorly. 5 ANA also happens to be the location, anatomically, where we can make the greatest impact with traditional rapid palatal expansion protocols (Fig 4). Recall that tradi-tional rapid palatal expansion results in a pyramidal shape of expansion from the superior-infe-rior (coronal) plane and, likewise, from the posterior-anterior (axial) plane, with the inferior and ante-rior exhibiting the greatest amount of expansion (Fig. 5). With rapid skeletal expansion, we can increase 10 Winter 2026 JAOS
Journal of the American Orthodontic Society Winter 2026: Page 10