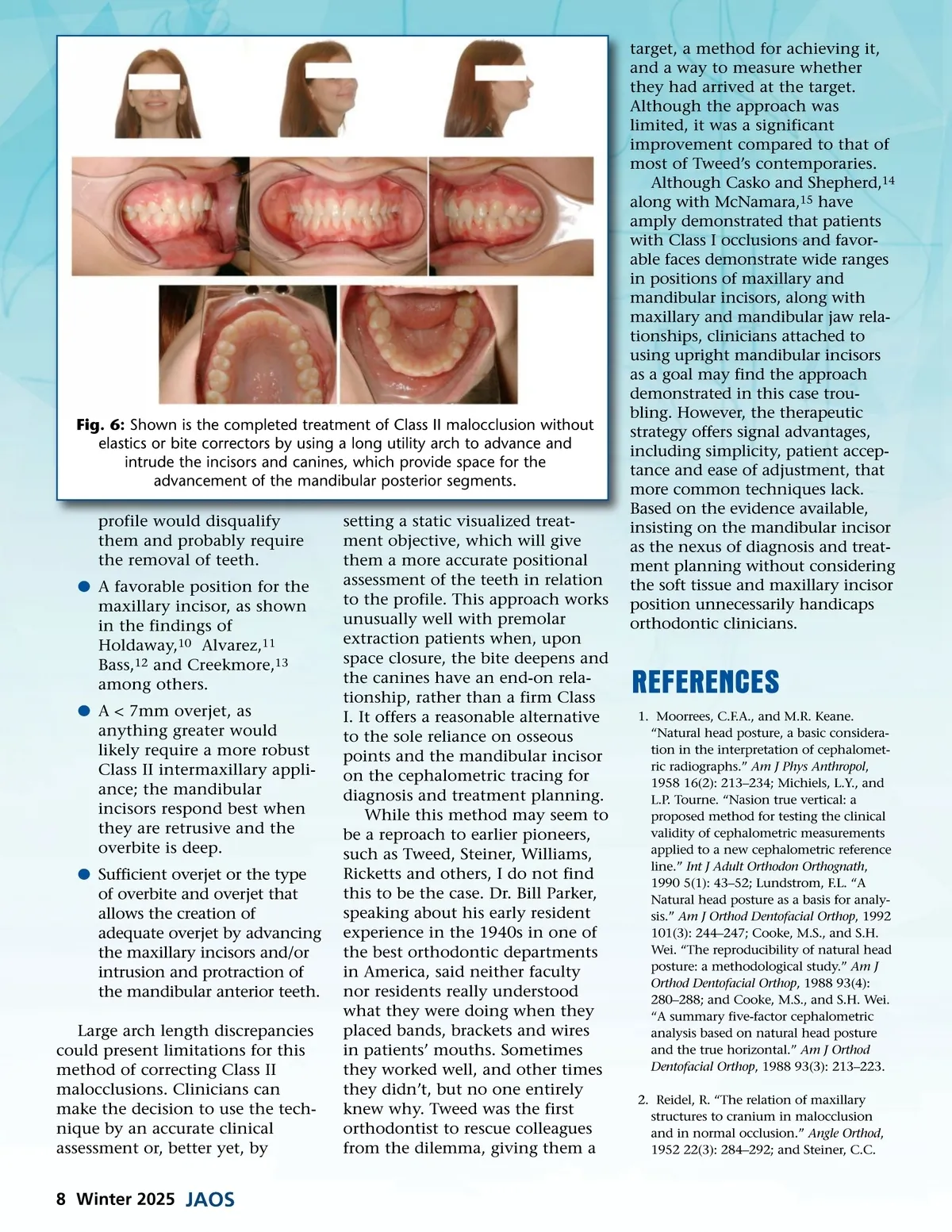
Fig. 6: Shown is the completed treatment of Class II malocclusion without elastics or bite correctors by using a long utility arch to advance and intrude the incisors and canines, which provide space for the advancement of the mandibular posterior segments. profile would disqualify them and probably require the removal of teeth. b A favorable position for the maxillary incisor, as shown in the findings of Holdaway, 10 Alvarez, 11 Bass, 12 and Creekmore, 13 among others. b A < 7mm overjet, as anything greater would likely require a more robust Class II intermaxillary appli-ance; the mandibular incisors respond best when they are retrusive and the overbite is deep. b Sufficient overjet or the type of overbite and overjet that allows the creation of adequate overjet by advancing the maxillary incisors and/or intrusion and protraction of the mandibular anterior teeth. Large arch length discrepancies could present limitations for this method of correcting Class II malocclusions. Clinicians can make the decision to use the tech-nique by an accurate clinical assessment or, better yet, by setting a static visualized treat-ment objective, which will give them a more accurate positional assessment of the teeth in relation to the profile. This approach works unusually well with premolar extraction patients when, upon space closure, the bite deepens and the canines have an end-on rela-tionship, rather than a firm Class I. It offers a reasonable alternative to the sole reliance on osseous points and the mandibular incisor on the cephalometric tracing for diagnosis and treatment planning. While this method may seem to be a reproach to earlier pioneers, such as Tweed, Steiner, Williams, Ricketts and others, I do not find this to be the case. Dr. Bill Parker, speaking about his early resident experience in the 1940s in one of the best orthodontic departments in America, said neither faculty nor residents really understood what they were doing when they placed bands, brackets and wires in patients’ mouths. Sometimes they worked well, and other times they didn’t, but no one entirely knew why. Tweed was the first orthodontist to rescue colleagues from the dilemma, giving them a target, a method for achieving it, and a way to measure whether they had arrived at the target. Although the approach was limited, it was a significant improvement compared to that of most of Tweed’s contemporaries. Although Casko and Shepherd, 14 along with McNamara, 15 have amply demonstrated that patients with Class I occlusions and favor-able faces demonstrate wide ranges in positions of maxillary and mandibular incisors, along with maxillary and mandibular jaw rela-tionships, clinicians attached to using upright mandibular incisors as a goal may find the approach demonstrated in this case trou-bling. However, the therapeutic strategy offers signal advantages, including simplicity, patient accep-tance and ease of adjustment, that more common techniques lack. Based on the evidence available, insisting on the mandibular incisor as the nexus of diagnosis and treat-ment planning without considering the soft tissue and maxillary incisor position unnecessarily handicaps orthodontic clinicians. REFERENCES 1. Moorrees, C.F.A., and M.R. Keane. “Natural head posture, a basic considera-tion in the interpretation of cephalomet-ric radiographs.” Am J Phys Anthropol , 1958 16(2): 213–234; Michiels, L.Y., and L.P. Tourne. “Nasion true vertical: a proposed method for testing the clinical validity of cephalometric measurements applied to a new cephalometric reference line.” Int J Adult Orthodon Orthognath , 1990 5(1): 43–52; Lundstrom, F.L. “A Natural head posture as a basis for analy-sis.” Am J Orthod Dentofacial Orthop , 1992 101(3): 244–247; Cooke, M.S., and S.H. Wei. “The reproducibility of natural head posture: a methodological study.” Am J Orthod Dentofacial Orthop , 1988 93(4): 280–288; and Cooke, M.S., and S.H. Wei. “A summary five-factor cephalometric analysis based on natural head posture and the true horizontal.” Am J Orthod Dentofacial Orthop , 1988 93(3): 213–223. 2. Reidel, R. “The relation of maxillary structures to cranium in malocclusion and in normal occlusion.” Angle Orthod , 1952 22(3): 284–292; and Steiner, C.C. 8 Winter 2025 JAOS
Journal of the American Orthodontic Society Winter 2025: Page 8