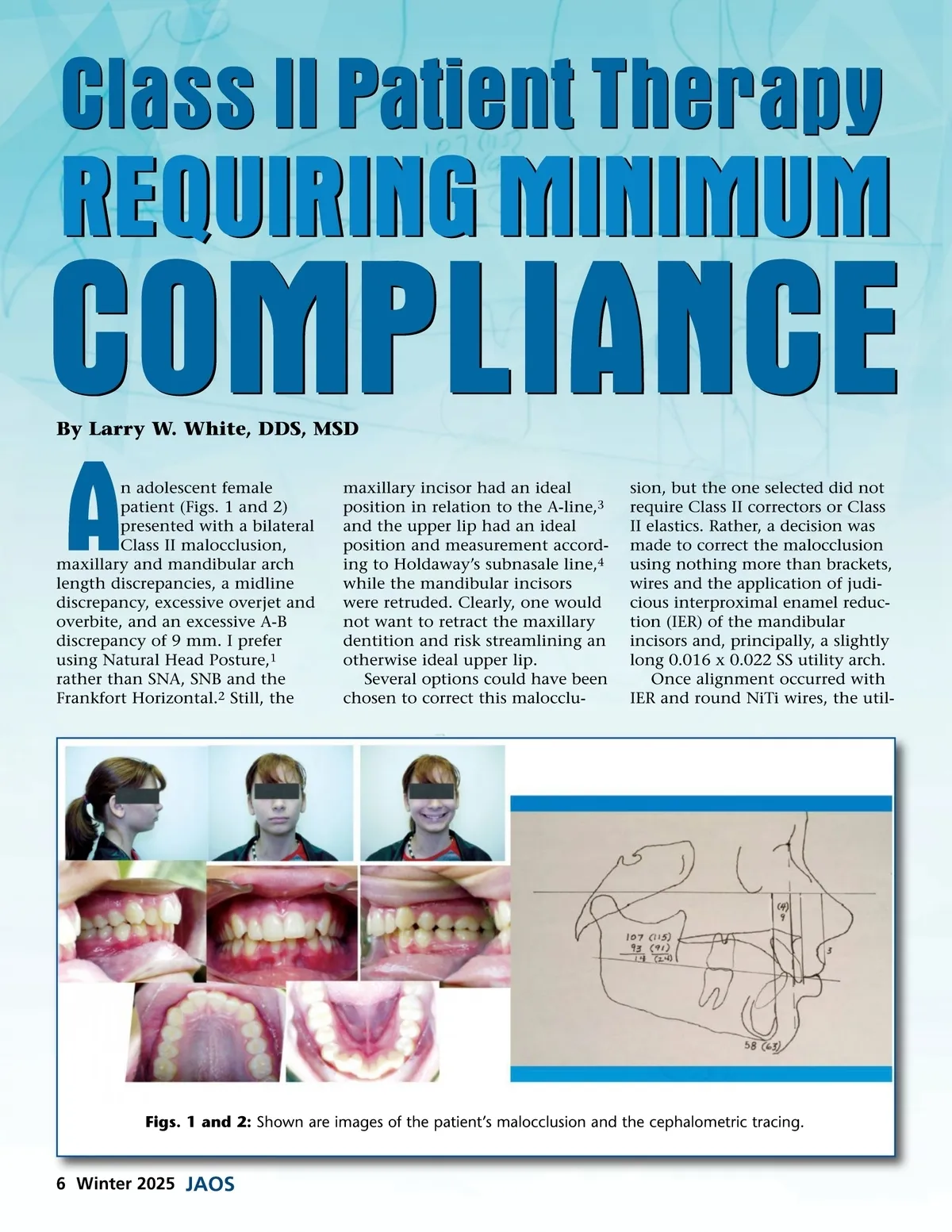
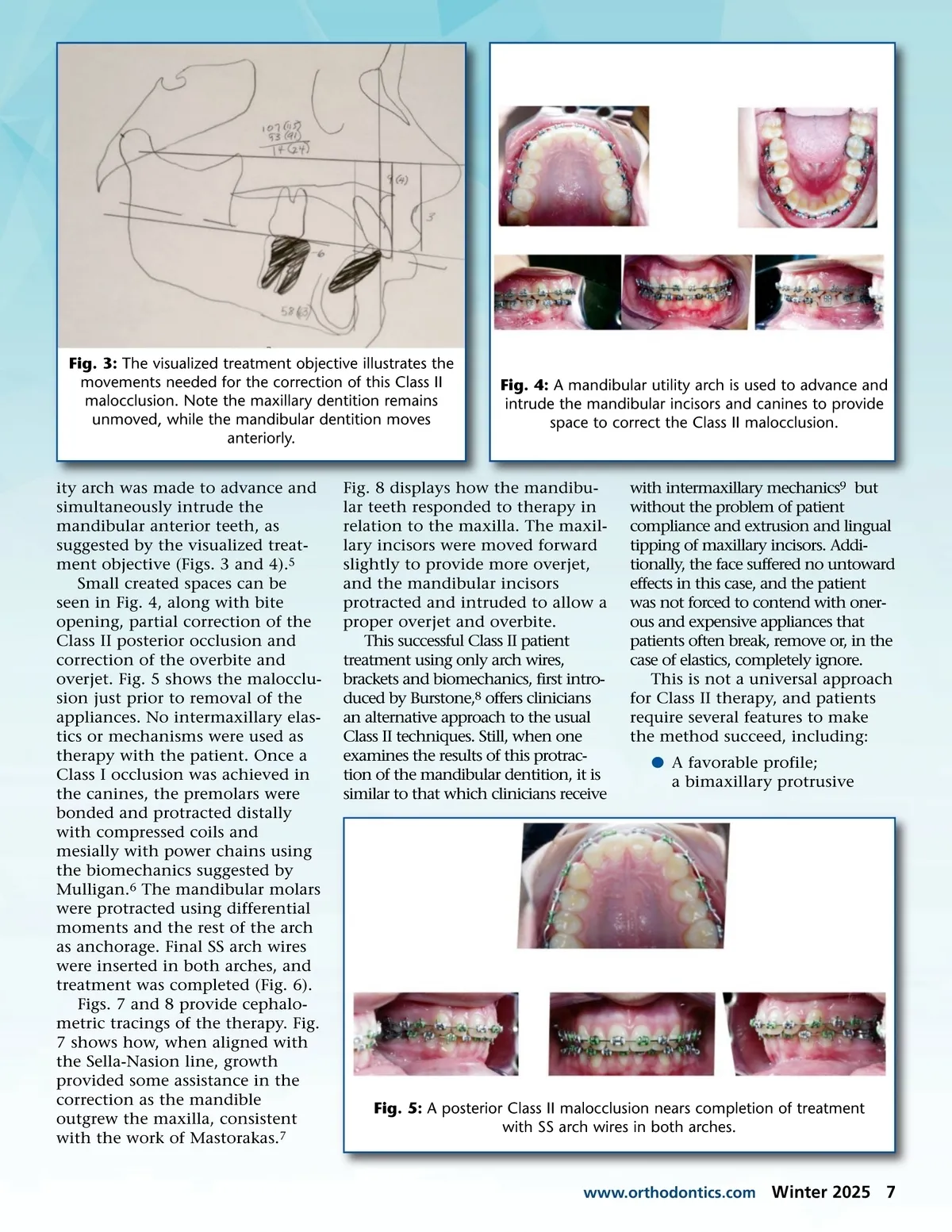
Fig. 3: The visualized treatment objective illustrates the movements needed for the correction of this Class II malocclusion. Note the maxillary dentition remains unmoved, while the mandibular dentition moves anteriorly. ity arch was made to advance and simultaneously intrude the mandibular anterior teeth, as suggested by the visualized treat-ment objective (Figs. 3 and 4). 5 Small created spaces can be seen in Fig. 4, along with bite opening, partial correction of the Class II posterior occlusion and correction of the overbite and overjet. Fig. 5 shows the malocclu-sion just prior to removal of the appliances. No intermaxillary elas-tics or mechanisms were used as therapy with the patient. Once a Class I occlusion was achieved in the canines, the premolars were bonded and protracted distally with compressed coils and mesially with power chains using the biomechanics suggested by Mulligan. 6 The mandibular molars were protracted using differential moments and the rest of the arch as anchorage. Final SS arch wires were inserted in both arches, and treatment was completed (Fig. 6). Figs. 7 and 8 provide cephalo-metric tracings of the therapy. Fig. 7 shows how, when aligned with the Sella-Nasion line, growth provided some assistance in the correction as the mandible outgrew the maxilla, consistent with the work of Mastorakas. 7 Fig. 4: A mandibular utility arch is used to advance and intrude the mandibular incisors and canines to provide space to correct the Class II malocclusion. Fig. 8 displays how the mandibu-lar teeth responded to therapy in relation to the maxilla. The maxil-lary incisors were moved forward slightly to provide more overjet, and the mandibular incisors protracted and intruded to allow a proper overjet and overbite. This successful Class II patient treatment using only arch wires, brackets and biomechanics, first intro-duced by Burstone, 8 offers clinicians an alternative approach to the usual Class II techniques. Still, when one examines the results of this protrac-tion of the mandibular dentition, it is similar to that which clinicians receive with intermaxillary mechanics 9 but without the problem of patient compliance and extrusion and lingual tipping of maxillary incisors. Addi-tionally, the face suffered no untoward effects in this case, and the patient was not forced to contend with oner-ous and expensive appliances that patients often break, remove or, in the case of elastics, completely ignore. This is not a universal approach for Class II therapy, and patients require several features to make the method succeed, including: b A favorable profile; a bimaxillary protrusive Fig. 5: A posterior Class II malocclusion nears completion of treatment with SS arch wires in both arches. www.orthodontics.com Winter 2025 7
Journal of the American Orthodontic Society Winter 2025: Page 7