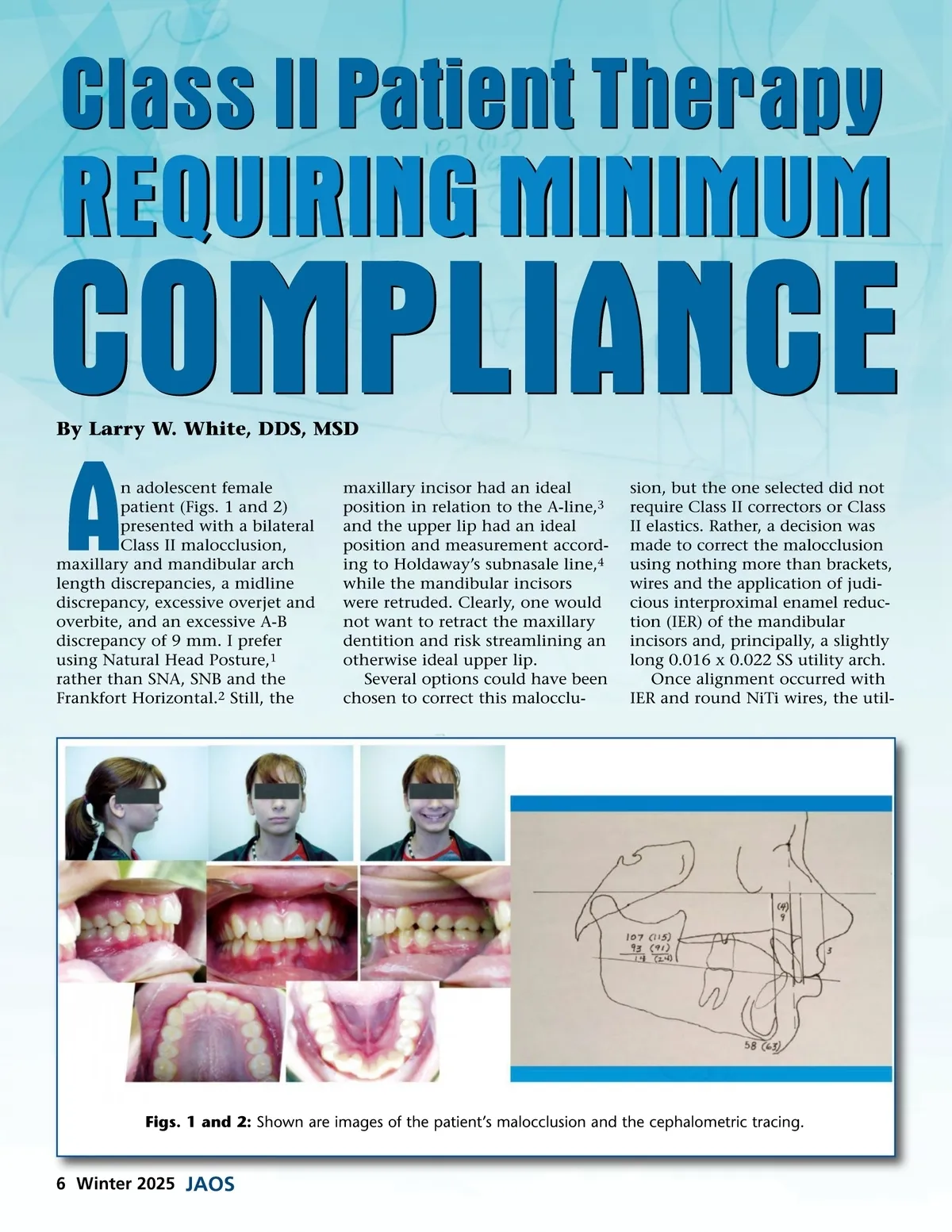
Class II Patient Therapy REQUIRING MINIMUM COMPLIANCE By Larry W. White, DDS, MSD A n adolescent female patient (Figs. 1 and 2) presented with a bilateral Class II malocclusion, maxillary and mandibular arch length discrepancies, a midline discrepancy, excessive overjet and overbite, and an excessive A-B discrepancy of 9 mm. I prefer using Natural Head Posture, 1 rather than SNA, SNB and the Frankfort Horizontal. 2 Still, the maxillary incisor had an ideal position in relation to the A-line, 3 and the upper lip had an ideal position and measurement accord-ing to Holdaway’s subnasale line, 4 while the mandibular incisors were retruded. Clearly, one would not want to retract the maxillary dentition and risk streamlining an otherwise ideal upper lip. Several options could have been chosen to correct this malocclu-sion, but the one selected did not require Class II correctors or Class II elastics. Rather, a decision was made to correct the malocclusion using nothing more than brackets, wires and the application of judi-cious interproximal enamel reduc-tion (IER) of the mandibular incisors and, principally, a slightly long 0.016 x 0.022 SS utility arch. Once alignment occurred with IER and round NiTi wires, the util-Figs. 1 and 2: Shown are images of the patient’s malocclusion and the cephalometric tracing. 6 Winter 2025 JAOS
Journal of the American Orthodontic Society Winter 2025: Page 6