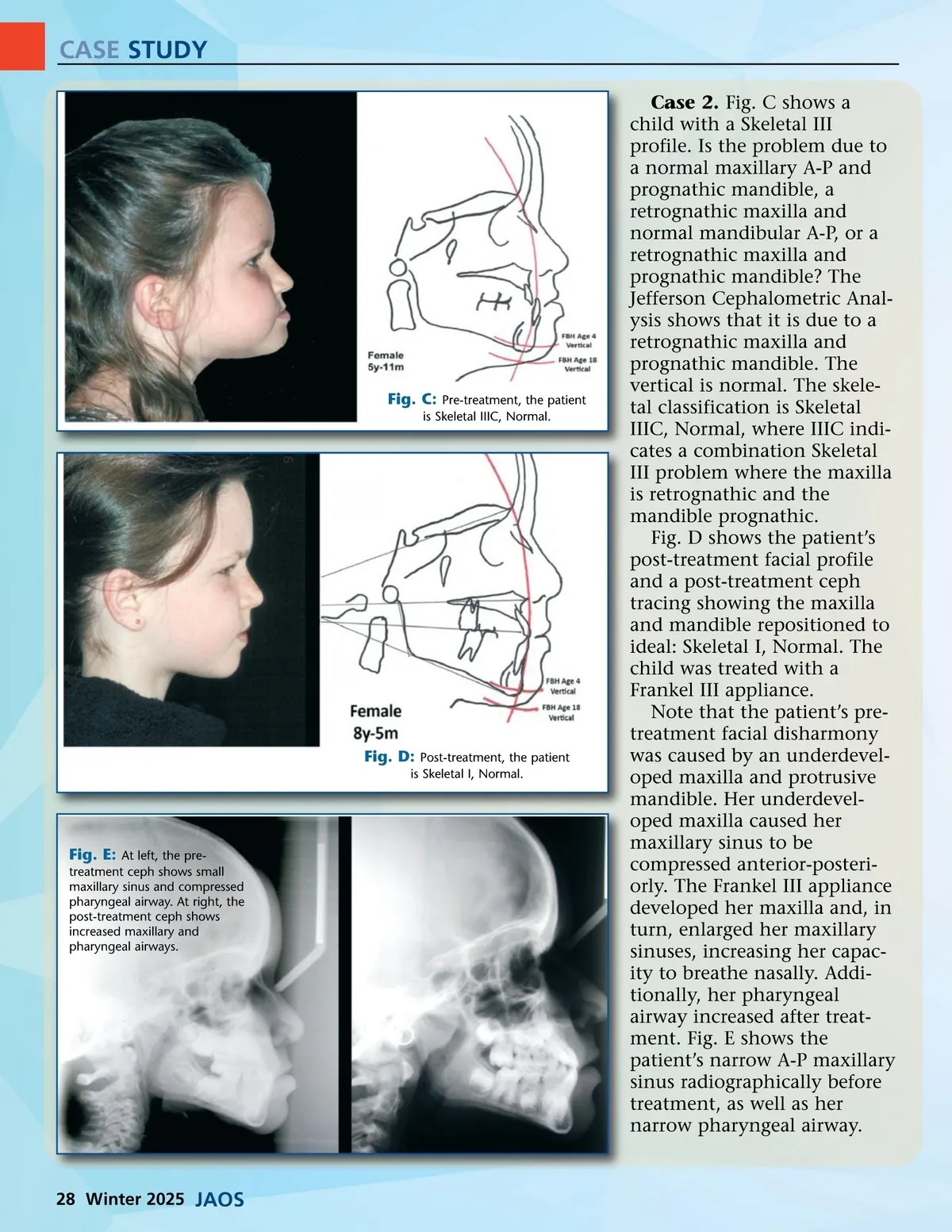
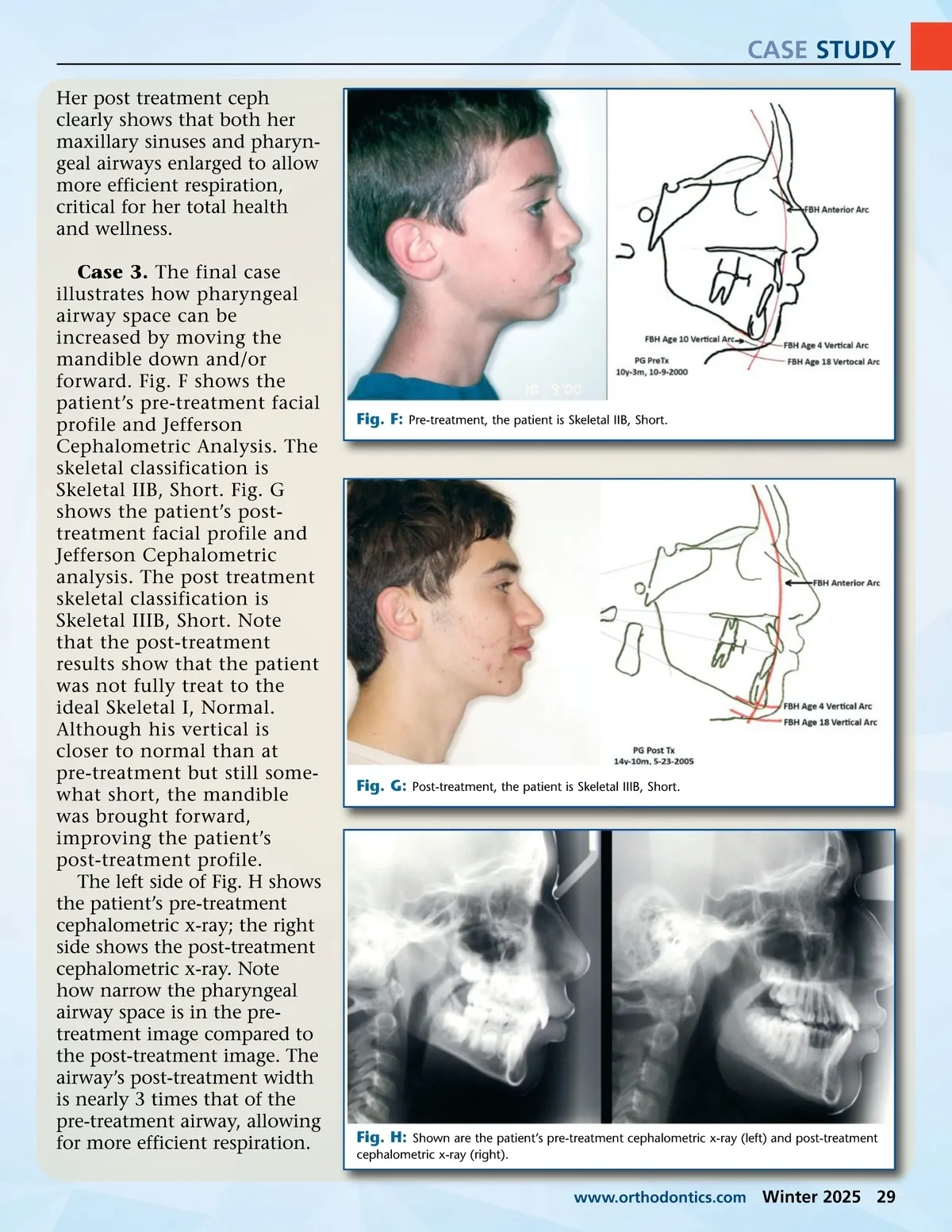
CASE STUDY Case 2. Fig. C shows a child with a Skeletal III profile. Is the problem due to a normal maxillary A-P and prognathic mandible, a retrognathic maxilla and normal mandibular A-P, or a retrognathic maxilla and prognathic mandible? The Jefferson Cephalometric Anal-ysis shows that it is due to a retrognathic maxilla and prognathic mandible. The vertical is normal. The skele-tal classification is Skeletal IIIC, Normal, where IIIC indi-cates a combination Skeletal III problem where the maxilla is retrognathic and the mandible prognathic. Fig. D shows the patient’s post-treatment facial profile and a post-treatment ceph tracing showing the maxilla and mandible repositioned to ideal: Skeletal I, Normal. The child was treated with a Frankel III appliance. Note that the patient’s pre-treatment facial disharmony was caused by an underdevel-oped maxilla and protrusive mandible. Her underdevel-oped maxilla caused her maxillary sinus to be compressed anterior-posteri-orly. The Frankel III appliance developed her maxilla and, in turn, enlarged her maxillary sinuses, increasing her capac-ity to breathe nasally. Addi-tionally, her pharyngeal airway increased after treat-ment. Fig. E shows the patient’s narrow A-P maxillary sinus radiographically before treatment, as well as her narrow pharyngeal airway. Fig. C: Pre-treatment, the patient is Skeletal IIIC, Normal. Fig. D: Post-treatment, the patient is Skeletal I, Normal. Fig. E: At left, the pre-treatment ceph shows small maxillary sinus and compressed pharyngeal airway. At right, the post-treatment ceph shows increased maxillary and pharyngeal airways. 28 Winter 2025 JAOS
Journal of the American Orthodontic Society Winter 2025: Page 28