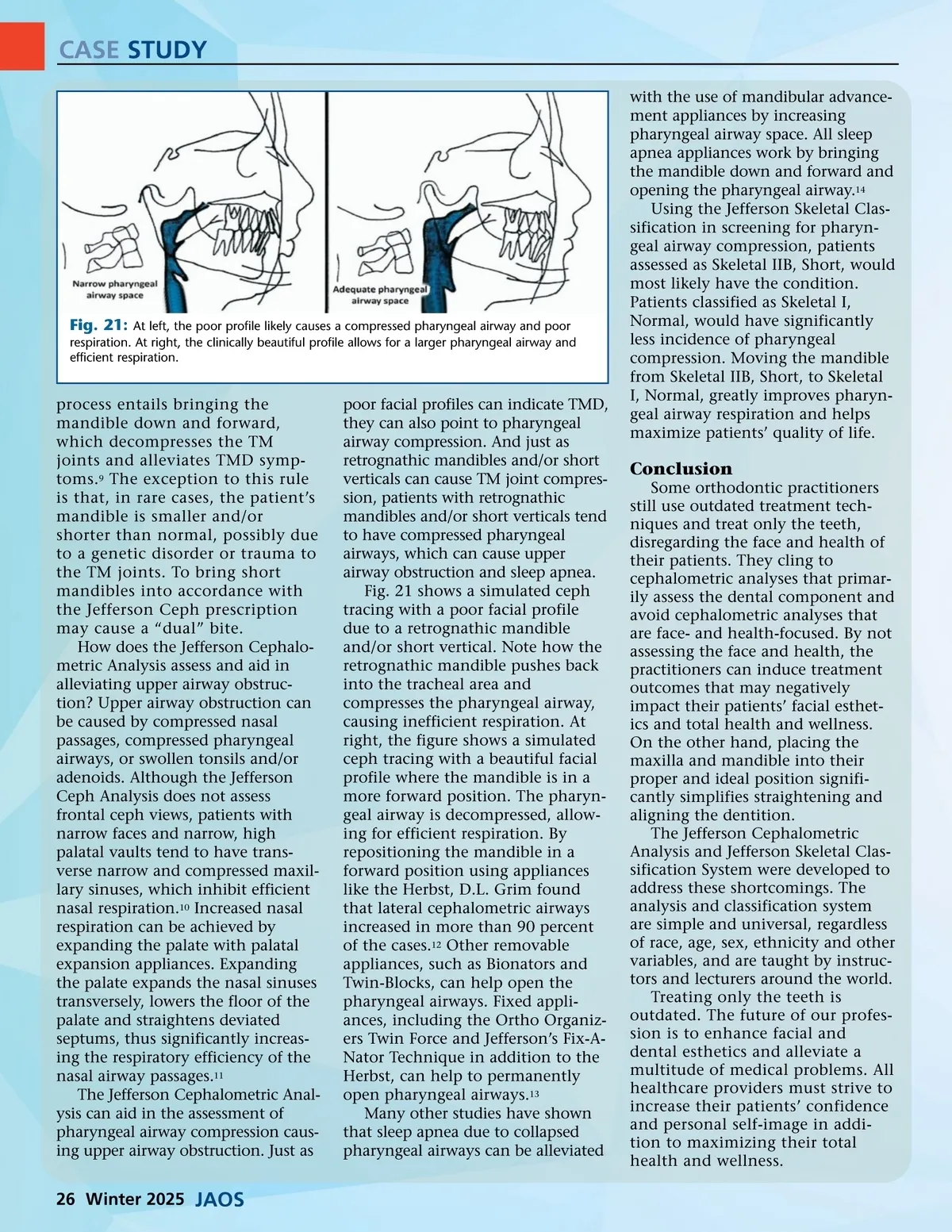
CASE STUDY with the use of mandibular advance-ment appliances by increasing pharyngeal airway space. All sleep apnea appliances work by bringing the mandible down and forward and opening the pharyngeal airway. 14 Using the Jefferson Skeletal Clas-sification in screening for pharyn-geal airway compression, patients assessed as Skeletal IIB, Short, would most likely have the condition. Patients classified as Skeletal I, Normal, would have significantly less incidence of pharyngeal compression. Moving the mandible from Skeletal IIB, Short, to Skeletal I, Normal, greatly improves pharyn-geal airway respiration and helps maximize patients’ quality of life. Fig. 21: At left, the poor profile likely causes a compressed pharyngeal airway and poor respiration. At right, the clinically beautiful profile allows for a larger pharyngeal airway and efficient respiration. process entails bringing the mandible down and forward, which decompresses the TM joints and alleviates TMD symp-toms. 9 The exception to this rule is that, in rare cases, the patient’s mandible is smaller and/or shorter than normal, possibly due to a genetic disorder or trauma to the TM joints. To bring short mandibles into accordance with the Jefferson Ceph prescription may cause a “dual” bite. How does the Jefferson Cephalo-metric Analysis assess and aid in alleviating upper airway obstruc-tion? Upper airway obstruction can be caused by compressed nasal passages, compressed pharyngeal airways, or swollen tonsils and/or adenoids. Although the Jefferson Ceph Analysis does not assess frontal ceph views, patients with narrow faces and narrow, high palatal vaults tend to have trans-verse narrow and compressed maxil-lary sinuses, which inhibit efficient nasal respiration. 10 Increased nasal respiration can be achieved by expanding the palate with palatal expansion appliances. Expanding the palate expands the nasal sinuses transversely, lowers the floor of the palate and straightens deviated septums, thus significantly increas-ing the respiratory efficiency of the nasal airway passages. 11 The Jefferson Cephalometric Anal-ysis can aid in the assessment of pharyngeal airway compression caus-ing upper airway obstruction. Just as poor facial profiles can indicate TMD, they can also point to pharyngeal airway compression. And just as retrognathic mandibles and/or short verticals can cause TM joint compres-sion, patients with retrognathic mandibles and/or short verticals tend to have compressed pharyngeal airways, which can cause upper airway obstruction and sleep apnea. Fig. 21 shows a simulated ceph tracing with a poor facial profile due to a retrognathic mandible and/or short vertical. Note how the retrognathic mandible pushes back into the tracheal area and compresses the pharyngeal airway, causing inefficient respiration. At right, the figure shows a simulated ceph tracing with a beautiful facial profile where the mandible is in a more forward position. The pharyn-geal airway is decompressed, allow-ing for efficient respiration. By repositioning the mandible in a forward position using appliances like the Herbst, D.L. Grim found that lateral cephalometric airways increased in more than 90 percent of the cases. 12 Other removable appliances, such as Bionators and Twin-Blocks, can help open the pharyngeal airways. Fixed appli-ances, including the Ortho Organiz-ers Twin Force and Jefferson’s Fix-A-Nator Technique in addition to the Herbst, can help to permanently open pharyngeal airways. 13 Many other studies have shown that sleep apnea due to collapsed pharyngeal airways can be alleviated Conclusion Some orthodontic practitioners still use outdated treatment tech-niques and treat only the teeth, disregarding the face and health of their patients. They cling to cephalometric analyses that primar-ily assess the dental component and avoid cephalometric analyses that are face-and health-focused. By not assessing the face and health, the practitioners can induce treatment outcomes that may negatively impact their patients’ facial esthet-ics and total health and wellness. On the other hand, placing the maxilla and mandible into their proper and ideal position signifi-cantly simplifies straightening and aligning the dentition. The Jefferson Cephalometric Analysis and Jefferson Skeletal Clas-sification System were developed to address these shortcomings. The analysis and classification system are simple and universal, regardless of race, age, sex, ethnicity and other variables, and are taught by instruc-tors and lecturers around the world. Treating only the teeth is outdated. The future of our profes-sion is to enhance facial and dental esthetics and alleviate a multitude of medical problems. All healthcare providers must strive to increase their patients’ confidence and personal self-image in addi-tion to maximizing their total health and wellness. 26 Winter 2025 JAOS
Journal of the American Orthodontic Society Winter 2025: Page 26