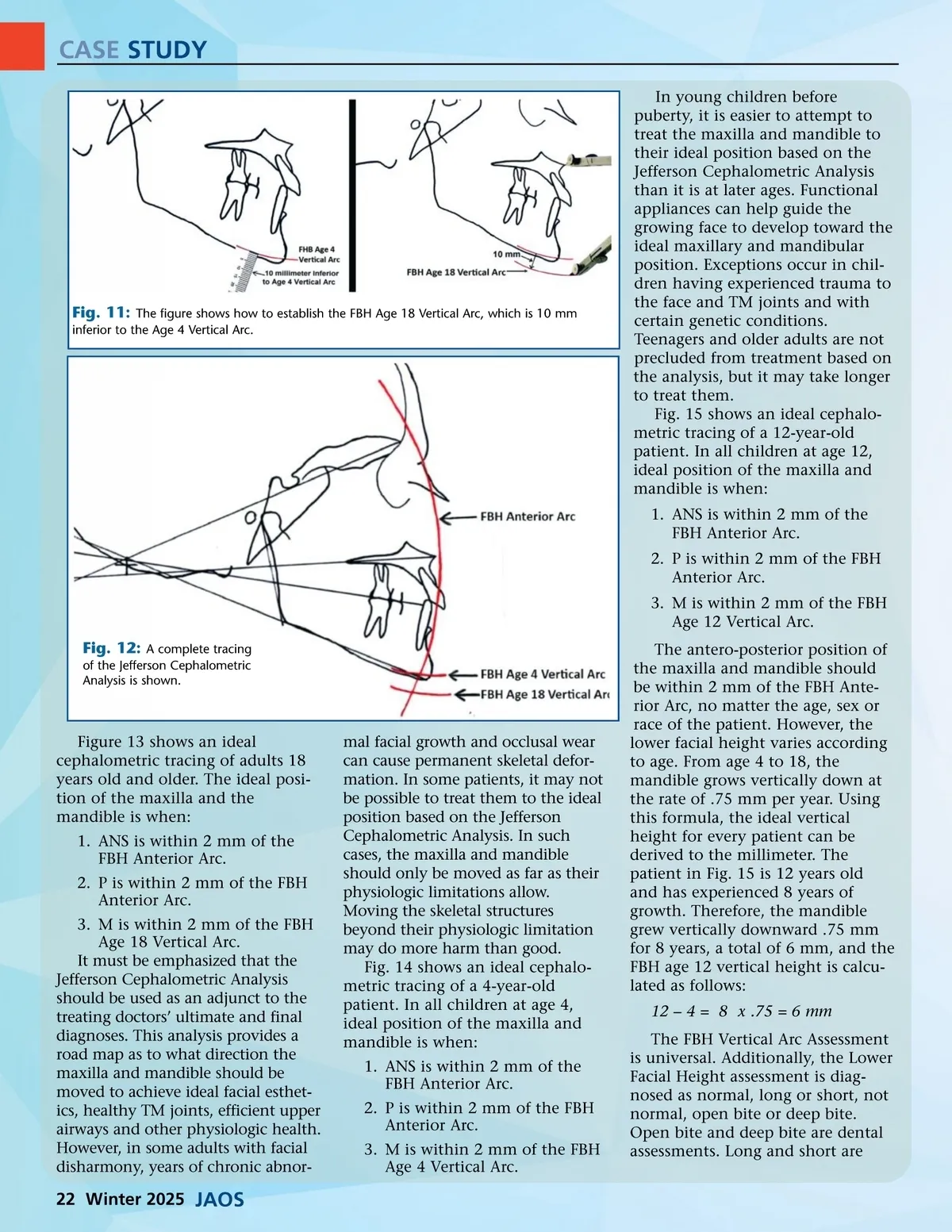
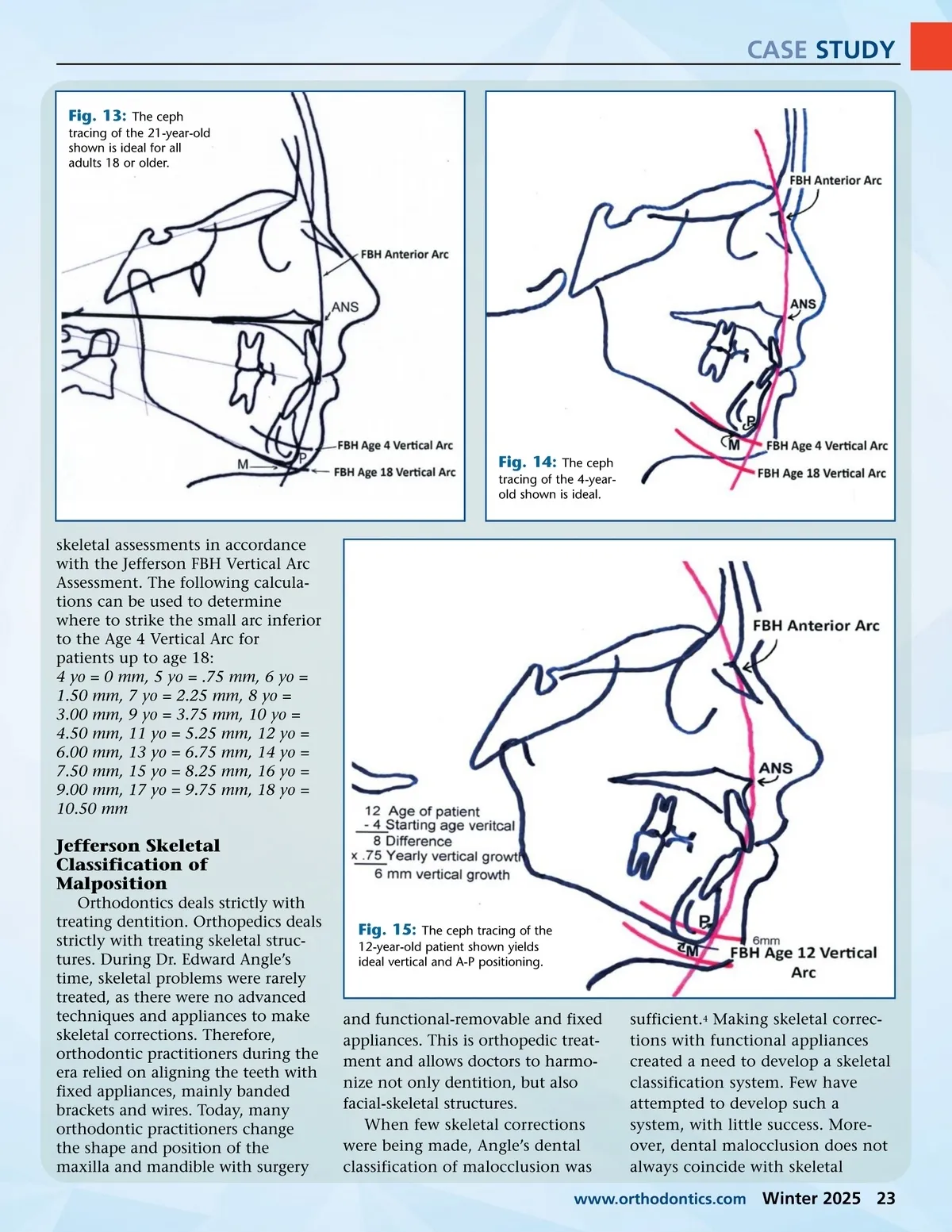
CASE STUDY Fig. 13: The ceph tracing of the 21-year-old shown is ideal for all adults 18 or older. Fig. 14: The ceph tracing of the 4-year-old shown is ideal. skeletal assessments in accordance with the Jefferson FBH Vertical Arc Assessment. The following calcula-tions can be used to determine where to strike the small arc inferior to the Age 4 Vertical Arc for patients up to age 18: 4 yo = 0 mm, 5 yo = .75 mm, 6 yo = 1.50 mm, 7 yo = 2.25 mm, 8 yo = 3.00 mm, 9 yo = 3.75 mm, 10 yo = 4.50 mm, 11 yo = 5.25 mm, 12 yo = 6.00 mm, 13 yo = 6.75 mm, 14 yo = 7.50 mm, 15 yo = 8.25 mm, 16 yo = 9.00 mm, 17 yo = 9.75 mm, 18 yo = 10.50 mm Jefferson Skeletal Classification of Malposition Orthodontics deals strictly with treating dentition. Orthopedics deals strictly with treating skeletal struc-tures. During Dr. Edward Angle’s time, skeletal problems were rarely treated, as there were no advanced techniques and appliances to make skeletal corrections. Therefore, orthodontic practitioners during the era relied on aligning the teeth with fixed appliances, mainly banded brackets and wires. Today, many orthodontic practitioners change the shape and position of the maxilla and mandible with surgery Fig. 15: The ceph tracing of the 12-year-old patient shown yields ideal vertical and A-P positioning. and functional-removable and fixed appliances. This is orthopedic treat-ment and allows doctors to harmo-nize not only dentition, but also facial-skeletal structures. When few skeletal corrections were being made, Angle’s dental classification of malocclusion was sufficient. 4 Making skeletal correc-tions with functional appliances created a need to develop a skeletal classification system. Few have attempted to develop such a system, with little success. More-over, dental malocclusion does not always coincide with skeletal www.orthodontics.com Winter 2025 23
Journal of the American Orthodontic Society Winter 2025: Page 23