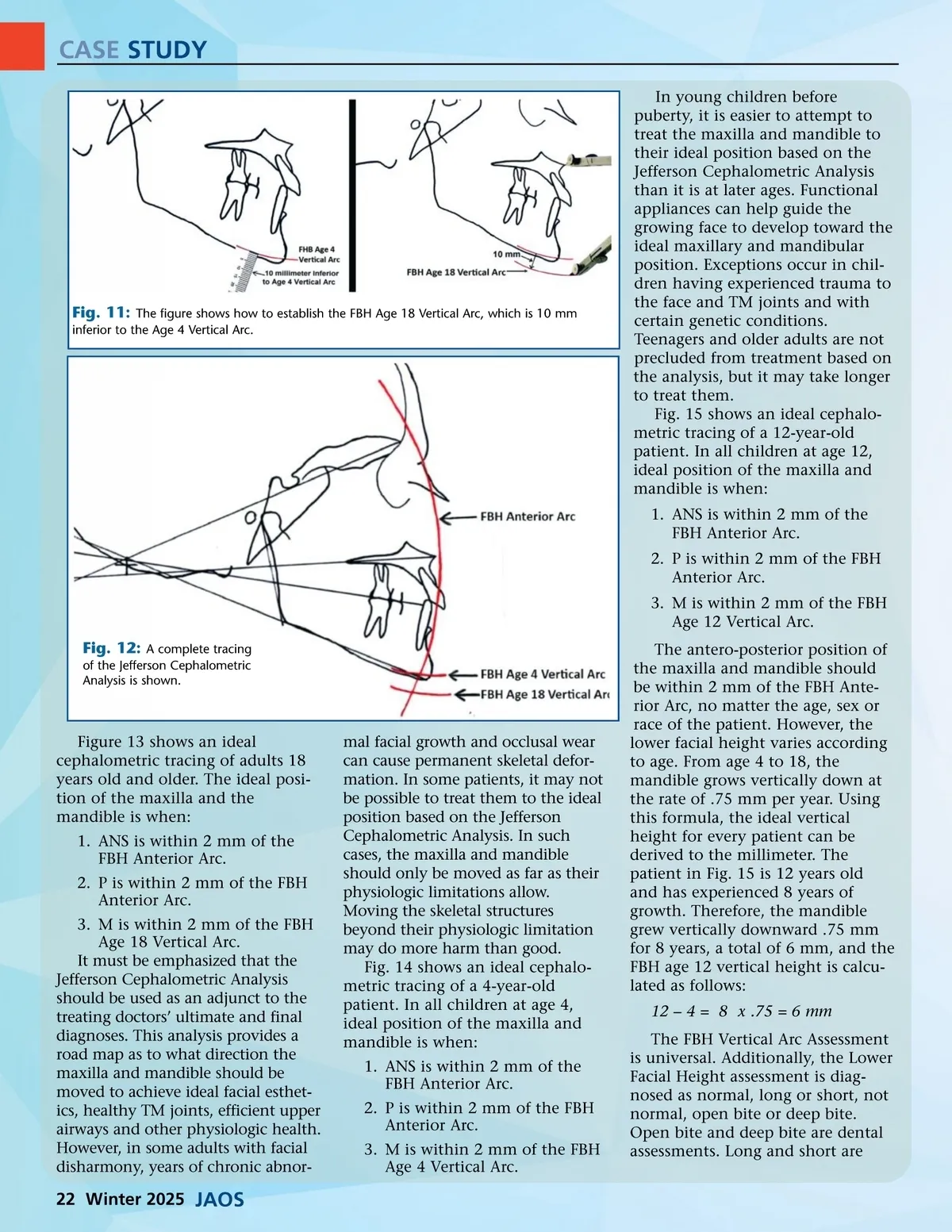
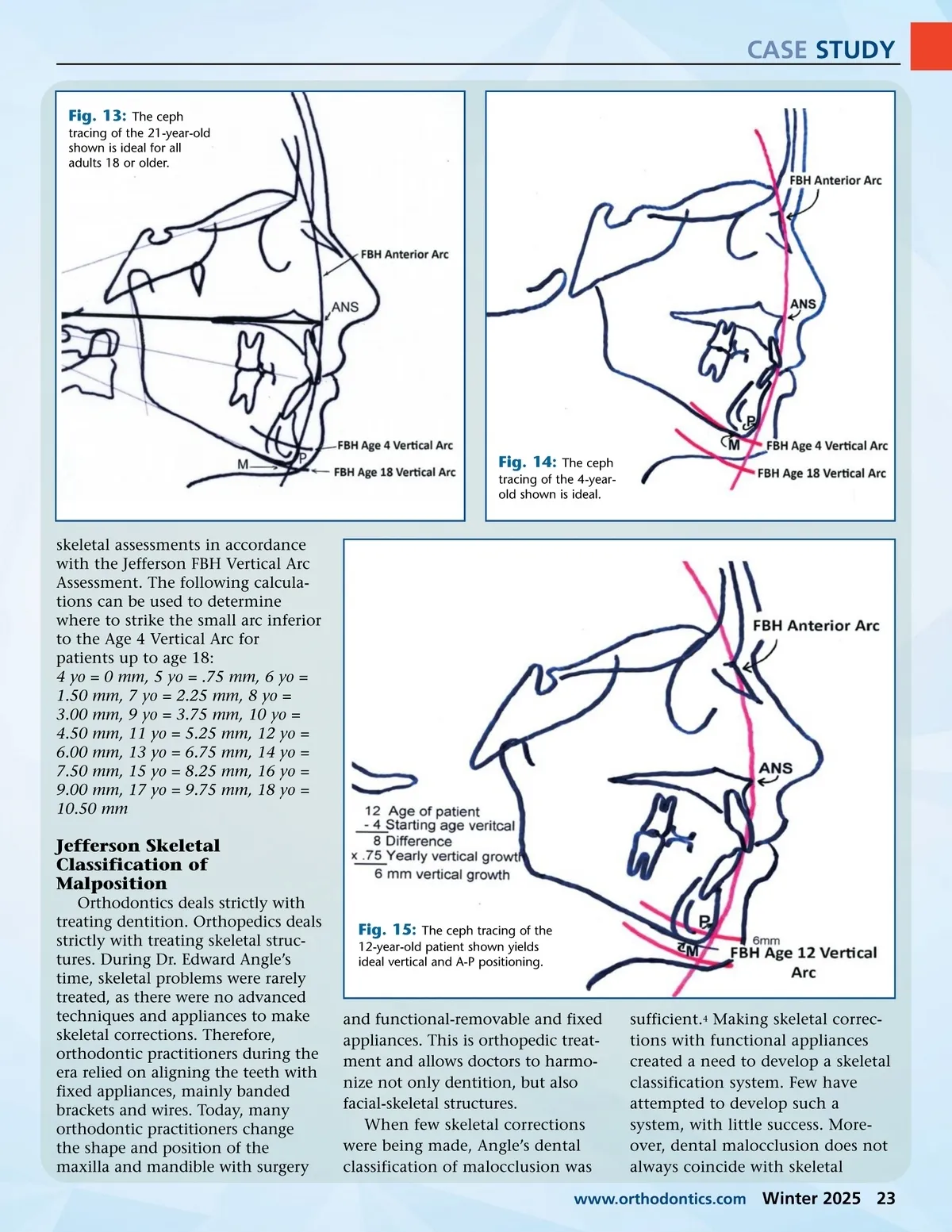
CASE STUDY In young children before puberty, it is easier to attempt to treat the maxilla and mandible to their ideal position based on the Jefferson Cephalometric Analysis than it is at later ages. Functional appliances can help guide the growing face to develop toward the ideal maxillary and mandibular position. Exceptions occur in chil-dren having experienced trauma to the face and TM joints and with certain genetic conditions. Teenagers and older adults are not precluded from treatment based on the analysis, but it may take longer to treat them. Fig. 15 shows an ideal cephalo-metric tracing of a 12-year-old patient. In all children at age 12, ideal position of the maxilla and mandible is when: 1. ANS is within 2 mm of the FBH Anterior Arc. 2. P is within 2 mm of the FBH Anterior Arc. 3. M is within 2 mm of the FBH Age 12 Vertical Arc. Fig. 12: A complete tracing of the Jefferson Cephalometric Analysis is shown. Fig. 11: The figure shows how to establish the FBH Age 18 Vertical Arc, which is 10 mm inferior to the Age 4 Vertical Arc. Figure 13 shows an ideal cephalometric tracing of adults 18 years old and older. The ideal posi-tion of the maxilla and the mandible is when: 1. ANS is within 2 mm of the FBH Anterior Arc. 2. P is within 2 mm of the FBH Anterior Arc. 3. M is within 2 mm of the FBH Age 18 Vertical Arc. It must be emphasized that the Jefferson Cephalometric Analysis should be used as an adjunct to the treating doctors’ ultimate and final diagnoses. This analysis provides a road map as to what direction the maxilla and mandible should be moved to achieve ideal facial esthet-ics, healthy TM joints, efficient upper airways and other physiologic health. However, in some adults with facial disharmony, years of chronic abnor-mal facial growth and occlusal wear can cause permanent skeletal defor-mation. In some patients, it may not be possible to treat them to the ideal position based on the Jefferson Cephalometric Analysis. In such cases, the maxilla and mandible should only be moved as far as their physiologic limitations allow. Moving the skeletal structures beyond their physiologic limitation may do more harm than good. Fig. 14 shows an ideal cephalo-metric tracing of a 4-year-old patient. In all children at age 4, ideal position of the maxilla and mandible is when: 1. ANS is within 2 mm of the FBH Anterior Arc. 2. P is within 2 mm of the FBH Anterior Arc. 3. M is within 2 mm of the FBH Age 4 Vertical Arc. The antero-posterior position of the maxilla and mandible should be within 2 mm of the FBH Ante-rior Arc, no matter the age, sex or race of the patient. However, the lower facial height varies according to age. From age 4 to 18, the mandible grows vertically down at the rate of .75 mm per year. Using this formula, the ideal vertical height for every patient can be derived to the millimeter. The patient in Fig. 15 is 12 years old and has experienced 8 years of growth. Therefore, the mandible grew vertically downward .75 mm for 8 years, a total of 6 mm, and the FBH age 12 vertical height is calcu-lated as follows: 12 – 4 = 8 x .75 = 6 mm The FBH Vertical Arc Assessment is universal. Additionally, the Lower Facial Height assessment is diag-nosed as normal, long or short, not normal, open bite or deep bite. Open bite and deep bite are dental assessments. Long and short are 22 Winter 2025 JAOS
Journal of the American Orthodontic Society Winter 2025: Page 22