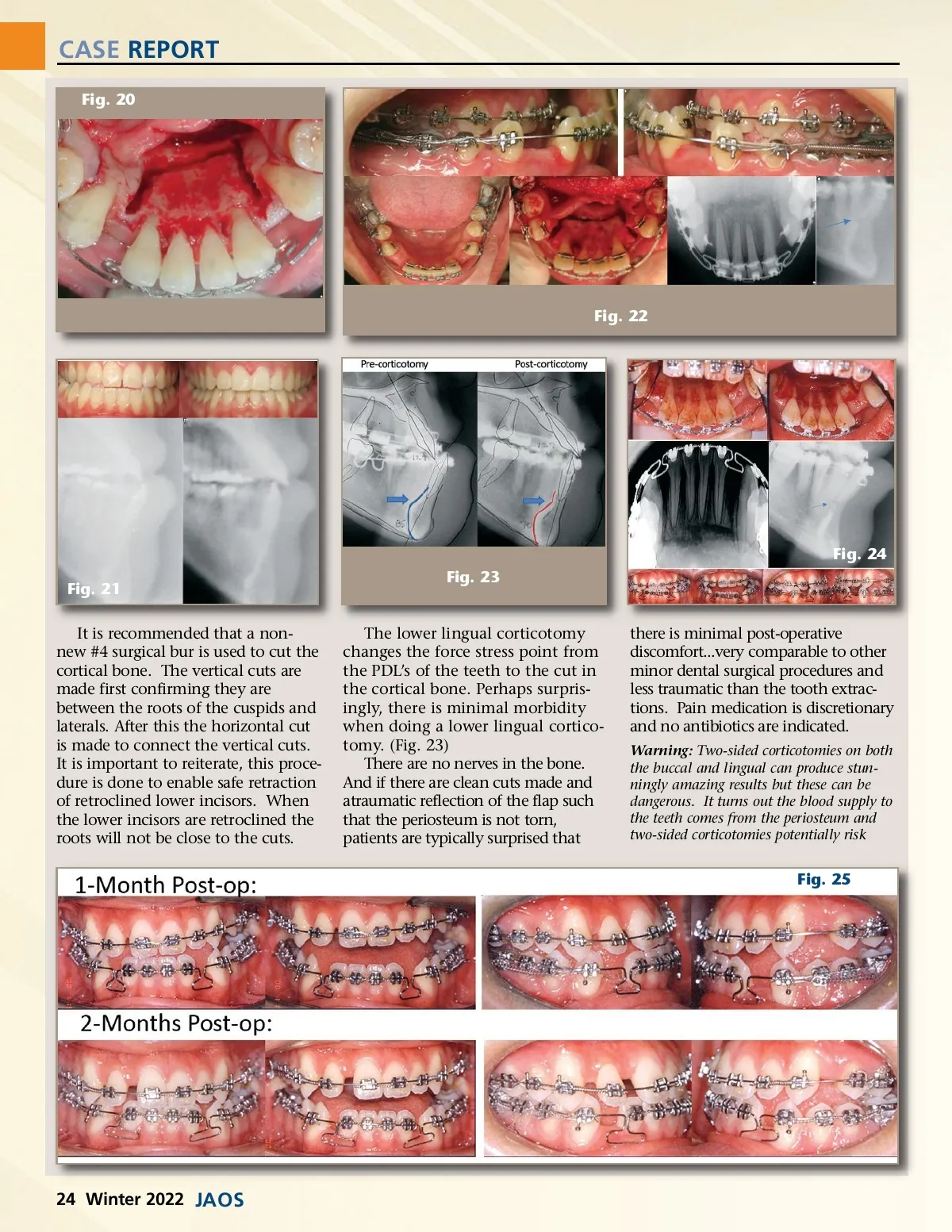
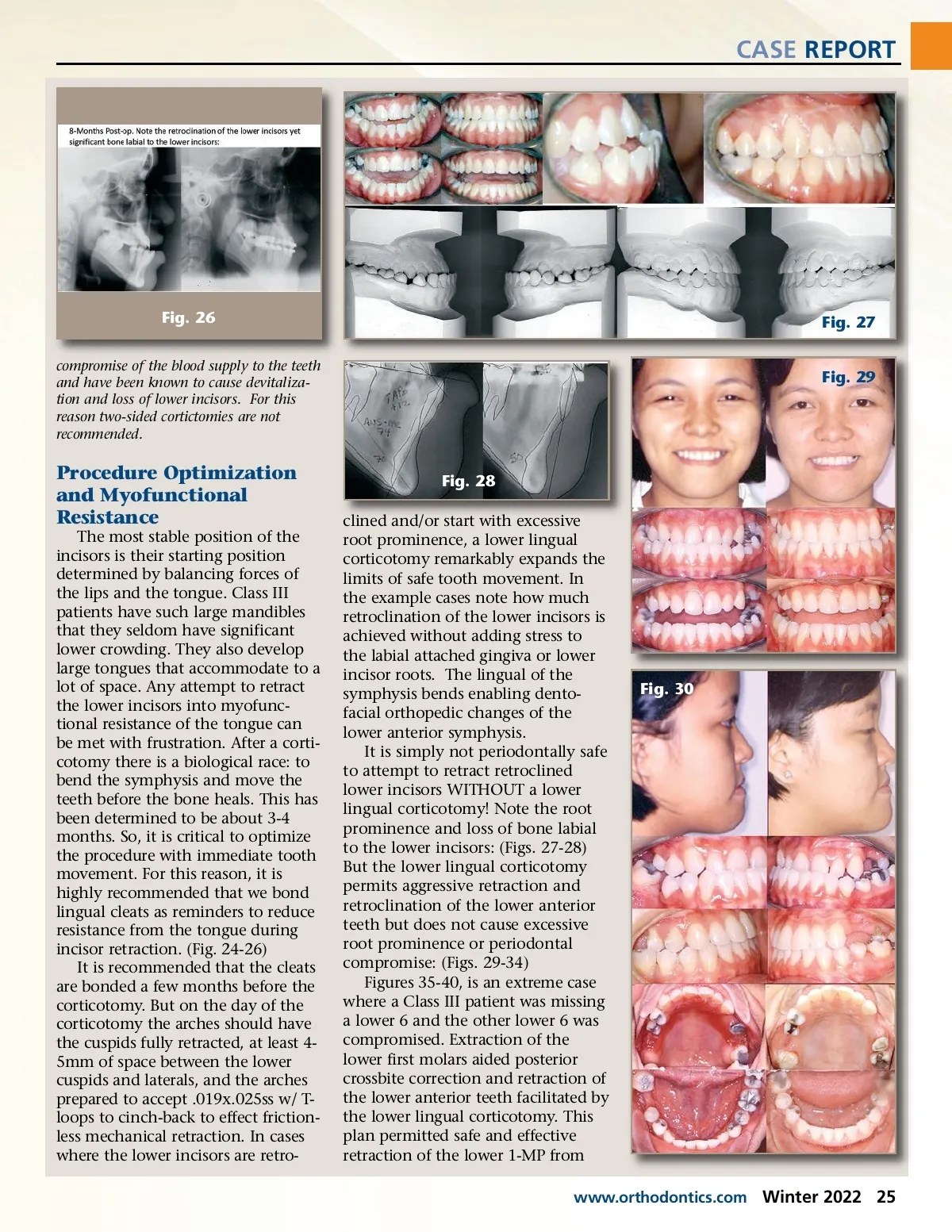
CASE REPORT Fig. 26 compromise of the blood supply to the teeth and have been known to cause devitaliza-tion and loss of lower incisors. For this reason two-sided cortictomies are not recommended. Fig. 27 Fig. 29 Procedure Optimization and Myofunctional Resistance The most stable position of the incisors is their starting position determined by balancing forces of the lips and the tongue. Class III patients have such large mandibles that they seldom have significant lower crowding. They also develop large tongues that accommodate to a lot of space. Any attempt to retract the lower incisors into myofunc-tional resistance of the tongue can be met with frustration. After a corti-cotomy there is a biological race: to bend the symphysis and move the teeth before the bone heals. This has been determined to be about 3-4 months. So, it is critical to optimize the procedure with immediate tooth movement. For this reason, it is highly recommended that we bond lingual cleats as reminders to reduce resistance from the tongue during incisor retraction. (Fig. 24-26) It is recommended that the cleats are bonded a few months before the corticotomy. But on the day of the corticotomy the arches should have the cuspids fully retracted, at least 4-5mm of space between the lower cuspids and laterals, and the arches prepared to accept .019x.025ss w/ T-loops to cinch-back to effect friction-less mechanical retraction. In cases where the lower incisors are retro-Fig. 28 clined and/or start with excessive root prominence, a lower lingual corticotomy remarkably expands the limits of safe tooth movement. In the example cases note how much retroclination of the lower incisors is achieved without adding stress to the labial attached gingiva or lower incisor roots. The lingual of the symphysis bends enabling dento-facial orthopedic changes of the lower anterior symphysis. It is simply not periodontally safe to attempt to retract retroclined lower incisors WITHOUT a lower lingual corticotomy! Note the root prominence and loss of bone labial to the lower incisors: (Figs. 27-28) But the lower lingual corticotomy permits aggressive retraction and retroclination of the lower anterior teeth but does not cause excessive root prominence or periodontal compromise: (Figs. 29-34) Figures 35-40, is an extreme case where a Class III patient was missing a lower 6 and the other lower 6 was compromised. Extraction of the lower first molars aided posterior crossbite correction and retraction of the lower anterior teeth facilitated by the lower lingual corticotomy. This plan permitted safe and effective retraction of the lower 1-MP from Fig. 30 www.orthodontics.com Winter 2022 25
Journal of the American Orthodontic Society Winter 2022: Page 25