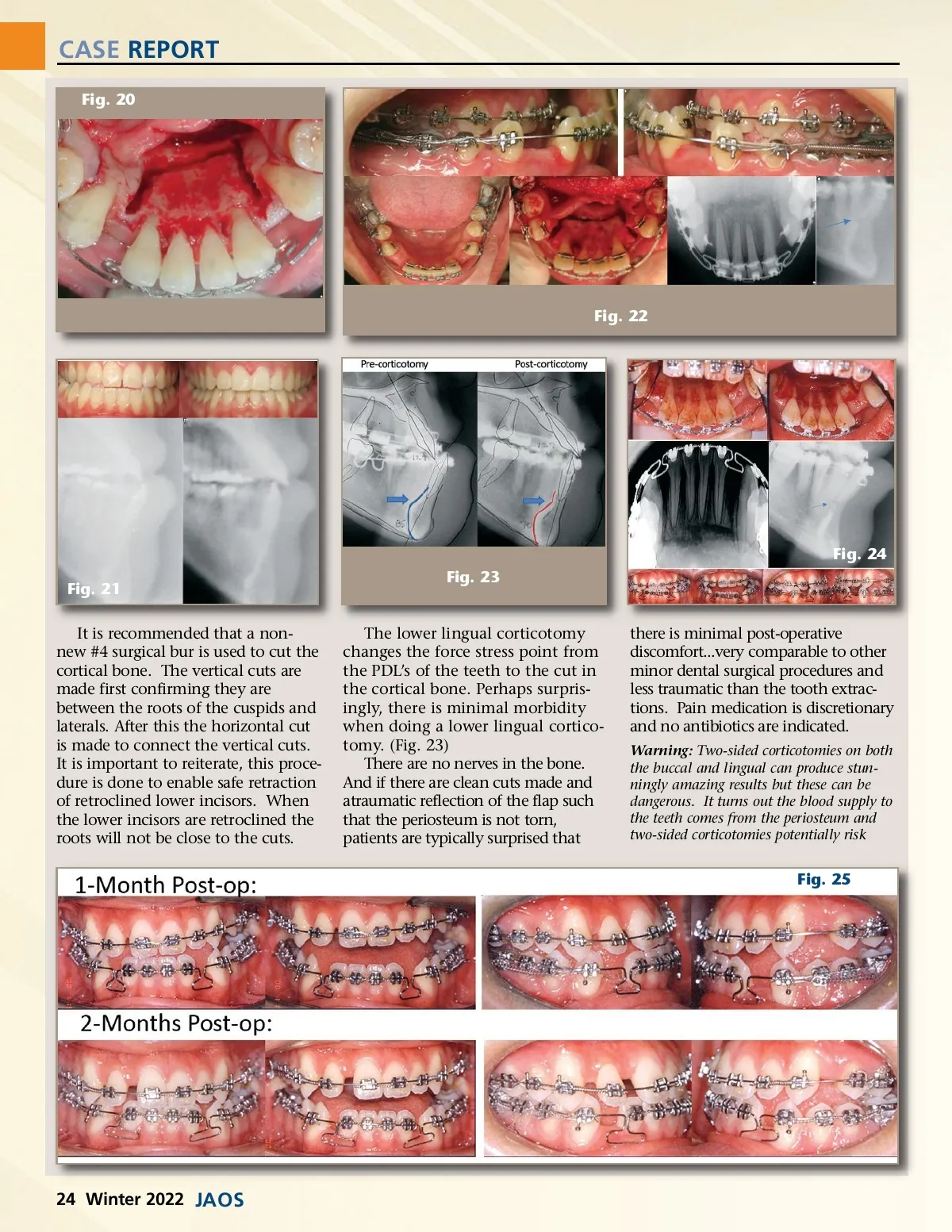
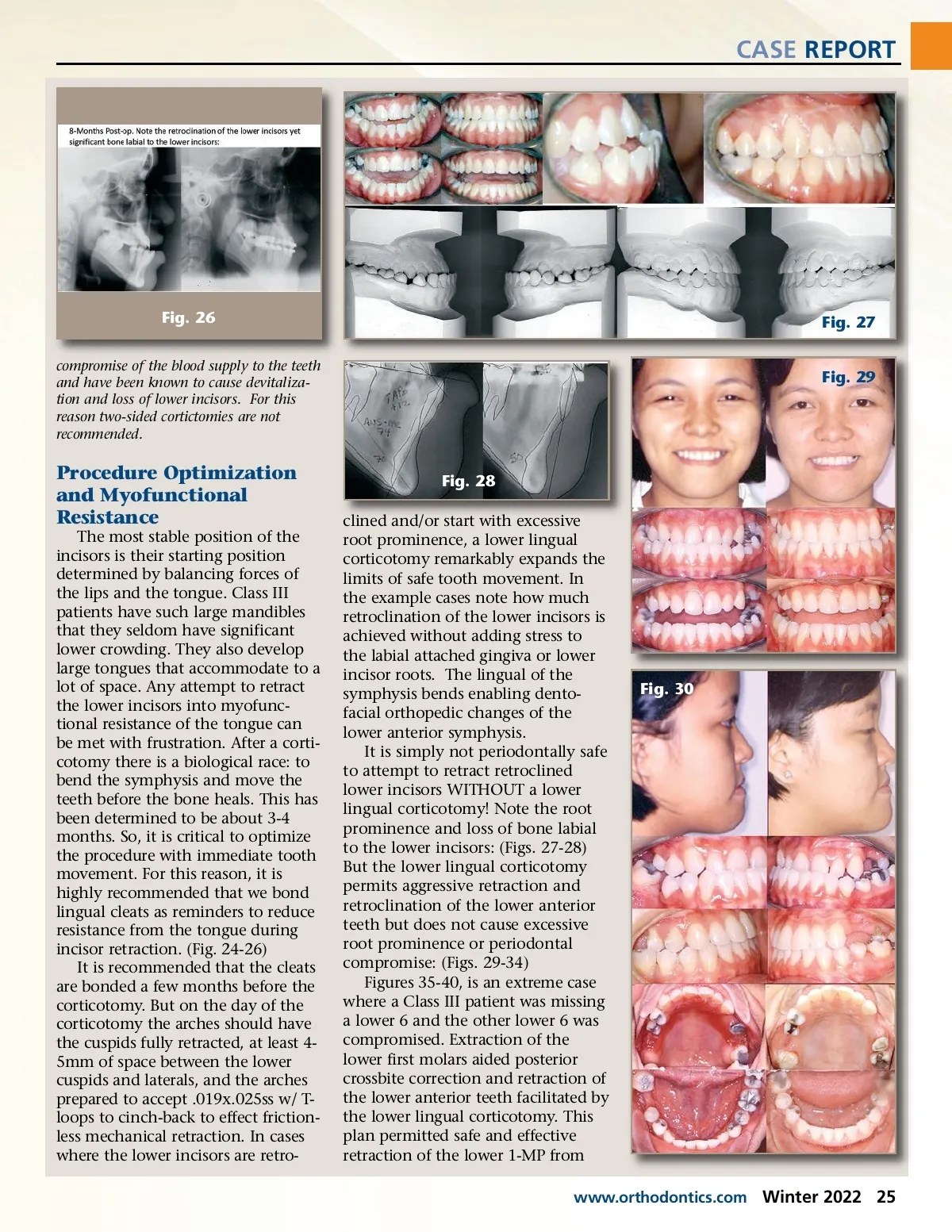
CASE REPORT Fig. 20 Fig. 22 Fig. 24 Fig. 21 It is recommended that a non-new #4 surgical bur is used to cut the cortical bone. The vertical cuts are made first confirming they are between the roots of the cuspids and laterals. After this the horizontal cut is made to connect the vertical cuts. It is important to reiterate, this proce-dure is done to enable safe retraction of retroclined lower incisors. When the lower incisors are retroclined the roots will not be close to the cuts. Fig. 23 The lower lingual corticotomy changes the force stress point from the PDL’s of the teeth to the cut in the cortical bone. Perhaps surpris-ingly, there is minimal morbidity when doing a lower lingual cortico-tomy. (Fig. 23) There are no nerves in the bone. And if there are clean cuts made and atraumatic reflection of the flap such that the periosteum is not torn, patients are typically surprised that there is minimal post-operative discomfort...very comparable to other minor dental surgical procedures and less traumatic than the tooth extrac-tions. Pain medication is discretionary and no antibiotics are indicated. Warning: Two-sided corticotomies on both the buccal and lingual can produce stun-ningly amazing results but these can be dangerous. It turns out the blood supply to the teeth comes from the periosteum and two-sided corticotomies potentially risk Fig. 25 24 Winter 2022 JAOS
Journal of the American Orthodontic Society Winter 2022: Page 24