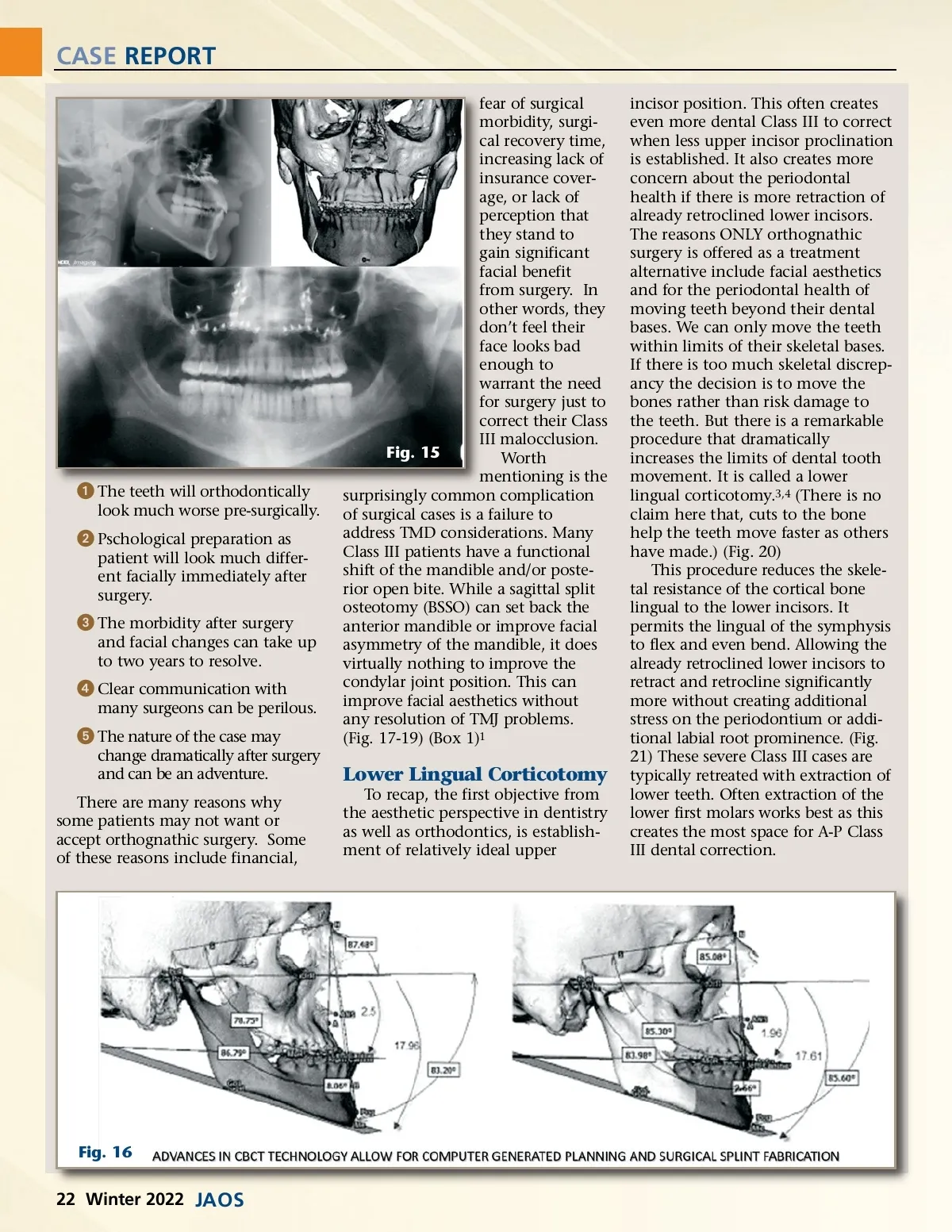
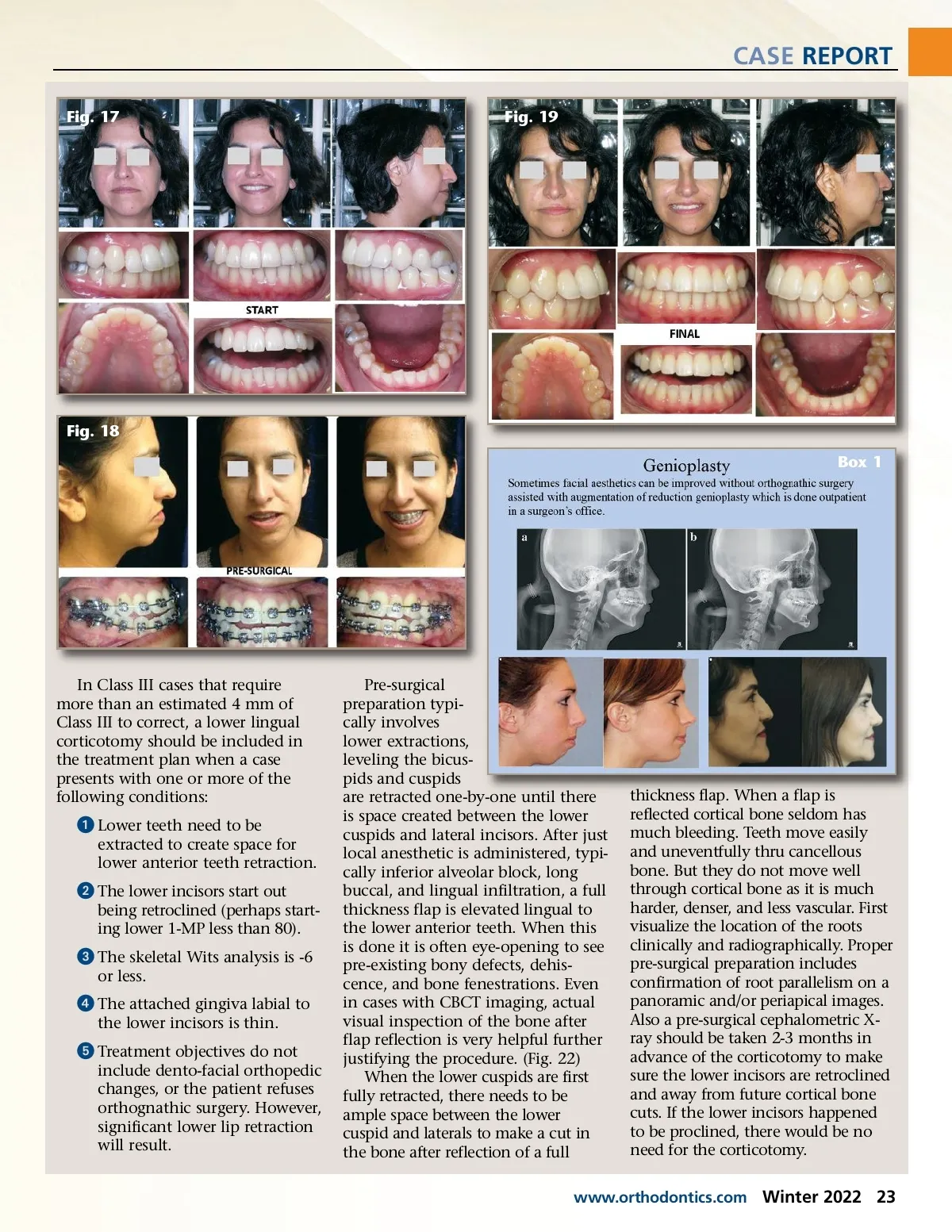
CASE REPORT Fig. 17 Fig. 19 Fig. 18 Box 1 In Class III cases that require more than an estimated 4 mm of Class III to correct, a lower lingual corticotomy should be included in the treatment plan when a case presents with one or more of the following conditions: ᕡ Lower teeth need to be extracted to create space for lower anterior teeth retraction. ᕢ The lower incisors start out being retroclined (perhaps start-ing lower 1-MP less than 80). ᕣ The skeletal Wits analysis is -6 or less. ᕤ The attached gingiva labial to the lower incisors is thin. ᕥ Treatment objectives do not include dento-facial orthopedic changes, or the patient refuses orthognathic surgery. However, significant lower lip retraction will result. Pre-surgical preparation typi-cally involves lower extractions, leveling the bicus-pids and cuspids are retracted one-by-one until there is space created between the lower cuspids and lateral incisors. After just local anesthetic is administered, typi-cally inferior alveolar block, long buccal, and lingual infiltration, a full thickness flap is elevated lingual to the lower anterior teeth. When this is done it is often eye-opening to see pre-existing bony defects, dehis-cence, and bone fenestrations. Even in cases with CBCT imaging, actual visual inspection of the bone after flap reflection is very helpful further justifying the procedure. (Fig. 22) When the lower cuspids are first fully retracted, there needs to be ample space between the lower cuspid and laterals to make a cut in the bone after reflection of a full thickness flap. When a flap is reflected cortical bone seldom has much bleeding. Teeth move easily and uneventfully thru cancellous bone. But they do not move well through cortical bone as it is much harder, denser, and less vascular. First visualize the location of the roots clinically and radiographically. Proper pre-surgical preparation includes confirmation of root parallelism on a panoramic and/or periapical images. Also a pre-surgical cephalometric X-ray should be taken 2-3 months in advance of the corticotomy to make sure the lower incisors are retroclined and away from future cortical bone cuts. If the lower incisors happened to be proclined, there would be no need for the corticotomy. www.orthodontics.com Winter 2022 23
Journal of the American Orthodontic Society Winter 2022: Page 23