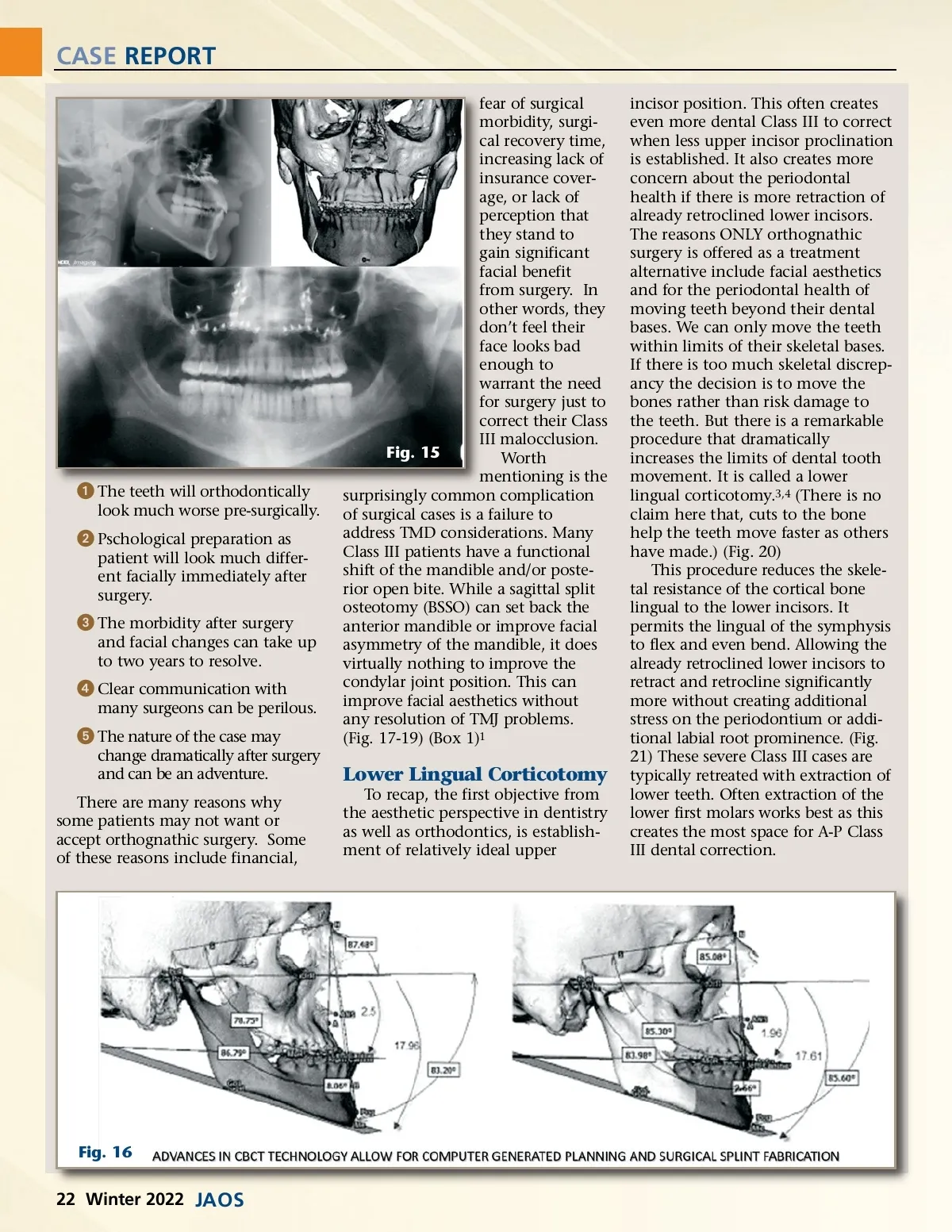
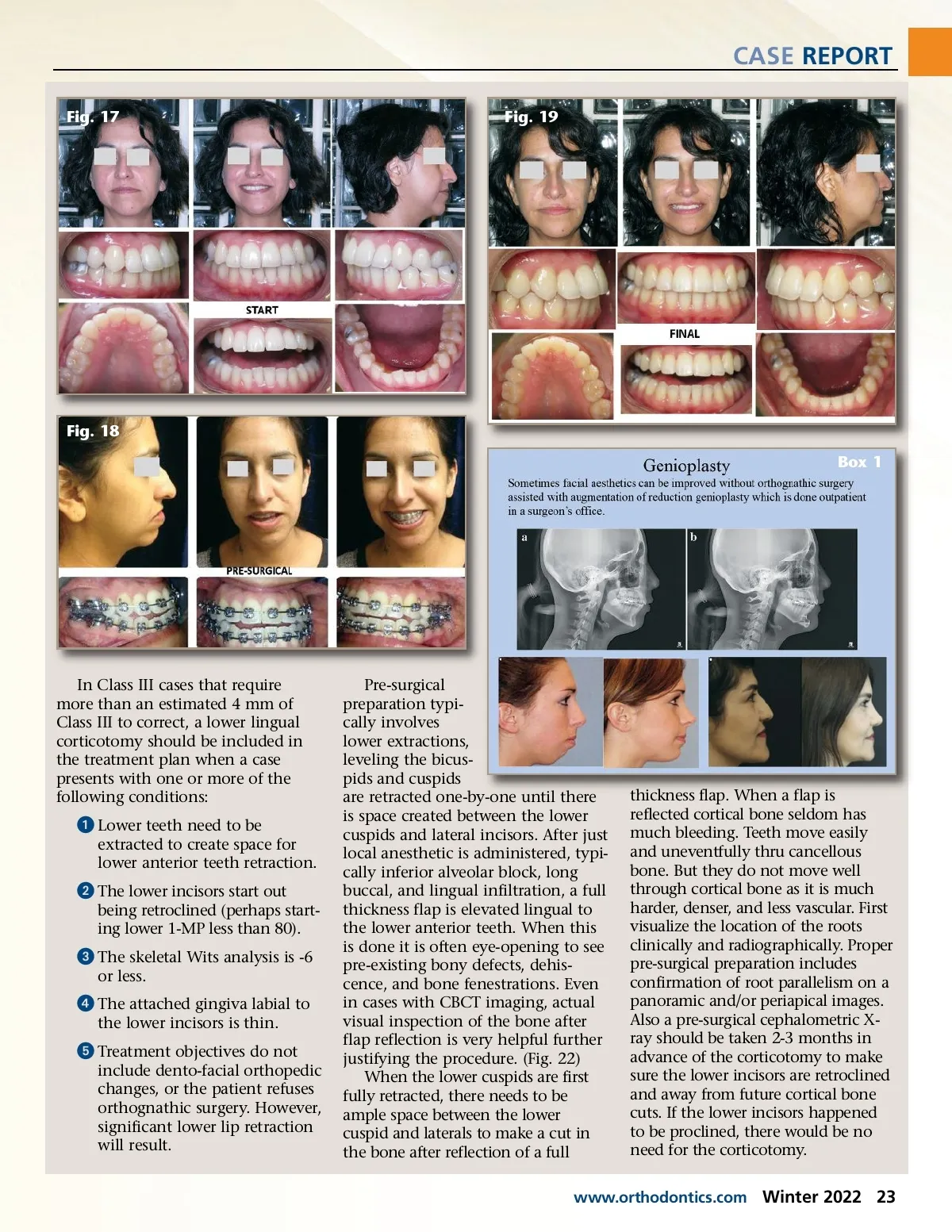
CASE REPORT fear of surgical morbidity, surgi-cal recovery time, increasing lack of insurance cover-age, or lack of perception that they stand to gain significant facial benefit from surgery. In other words, they don’t feel their face looks bad enough to warrant the need for surgery just to correct their Class III malocclusion. Fig. 15 Worth mentioning is the surprisingly common complication of surgical cases is a failure to address TMD considerations. Many Class III patients have a functional shift of the mandible and/or poste-rior open bite. While a sagittal split osteotomy (BSSO) can set back the anterior mandible or improve facial asymmetry of the mandible, it does virtually nothing to improve the condylar joint position. This can improve facial aesthetics without any resolution of TMJ problems. (Fig. 17-19) (Box 1) 1 incisor position. This often creates even more dental Class III to correct when less upper incisor proclination is established. It also creates more concern about the periodontal health if there is more retraction of already retroclined lower incisors. The reasons ONLY orthognathic surgery is offered as a treatment alternative include facial aesthetics and for the periodontal health of moving teeth beyond their dental bases. We can only move the teeth within limits of their skeletal bases. If there is too much skeletal discrep-ancy the decision is to move the bones rather than risk damage to the teeth. But there is a remarkable procedure that dramatically increases the limits of dental tooth movement. It is called a lower lingual corticotomy. 3,4 (There is no claim here that, cuts to the bone help the teeth move faster as others have made.) (Fig. 20) This procedure reduces the skele-tal resistance of the cortical bone lingual to the lower incisors. It permits the lingual of the symphysis to flex and even bend. Allowing the already retroclined lower incisors to retract and retrocline significantly more without creating additional stress on the periodontium or addi-tional labial root prominence. (Fig. 21) These severe Class III cases are typically retreated with extraction of lower teeth. Often extraction of the lower first molars works best as this creates the most space for A-P Class III dental correction. ᕡ The teeth will orthodontically look much worse pre-surgically. ᕢ Pschological preparation as patient will look much differ-ent facially immediately after surgery. ᕣ The morbidity after surgery and facial changes can take up to two years to resolve. ᕤ Clear communication with many surgeons can be perilous. ᕥ The nature of the case may change dramatically after surgery and can be an adventure. There are many reasons why some patients may not want or accept orthognathic surgery. Some of these reasons include financial, Lower Lingual Corticotomy To recap, the first objective from the aesthetic perspective in dentistry as well as orthodontics, is establish-ment of relatively ideal upper Fig. 16 22 Winter 2022 JAOS
Journal of the American Orthodontic Society Winter 2022: Page 22