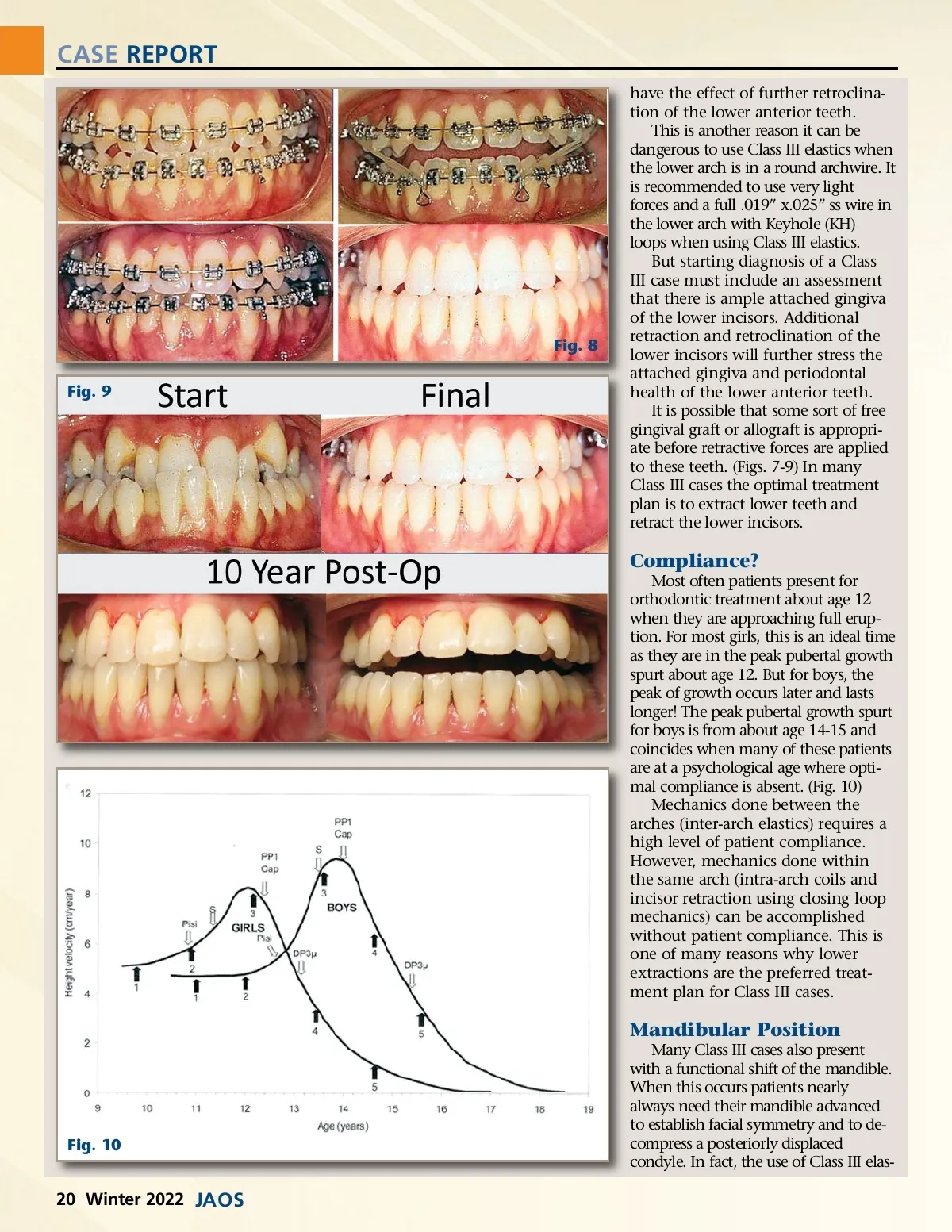
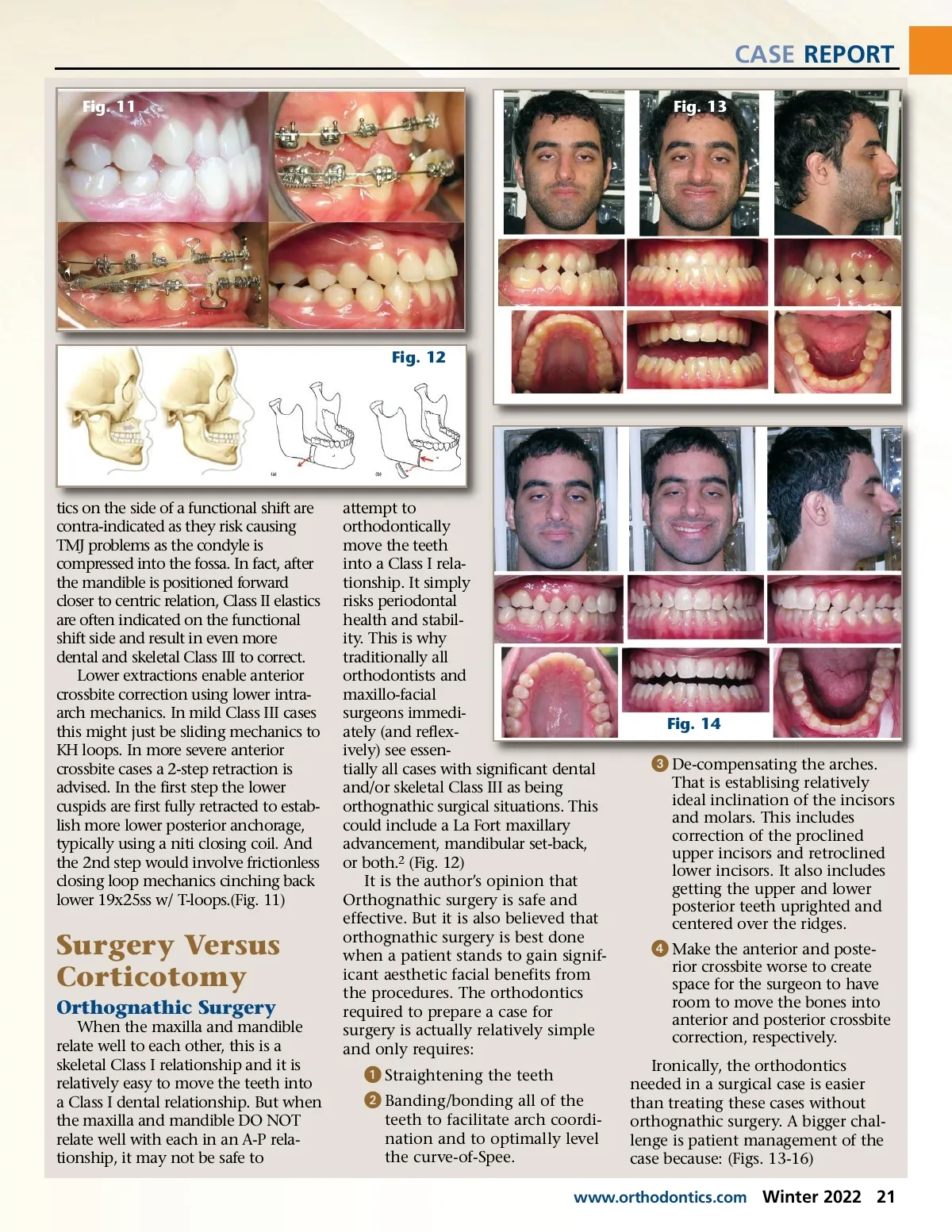
CASE REPORT Fig. 11 Fig. 13 Fig. 12 tics on the side of a functional shift are contra-indicated as they risk causing TMJ problems as the condyle is compressed into the fossa. In fact, after the mandible is positioned forward closer to centric relation, Class II elastics are often indicated on the functional shift side and result in even more dental and skeletal Class III to correct. Lower extractions enable anterior crossbite correction using lower intra-arch mechanics. In mild Class III cases this might just be sliding mechanics to KH loops. In more severe anterior crossbite cases a 2-step retraction is advised. In the first step the lower cuspids are first fully retracted to estab-lish more lower posterior anchorage, typically using a niti closing coil. And the 2nd step would involve frictionless closing loop mechanics cinching back lower 19x25ss w/ T-loops.(Fig. 11) Surgery Versus Corticotomy Orthognathic Surgery When the maxilla and mandible relate well to each other, this is a skeletal Class I relationship and it is relatively easy to move the teeth into a Class I dental relationship. But when the maxilla and mandible DO NOT relate well with each in an A-P rela-tionship, it may not be safe to attempt to orthodontically move the teeth into a Class I rela-tionship. It simply risks periodontal health and stabil-ity. This is why traditionally all orthodontists and maxillo-facial surgeons immedi-ately (and reflex-ively) see essen-tially all cases with significant dental and/or skeletal Class III as being orthognathic surgical situations. This could include a La Fort maxillary advancement, mandibular set-back, or both. 2 (Fig. 12) It is the author’s opinion that Orthognathic surgery is safe and effective. But it is also believed that orthognathic surgery is best done when a patient stands to gain signif-icant aesthetic facial benefits from the procedures. The orthodontics required to prepare a case for surgery is actually relatively simple and only requires: Fig. 14 ᕣ De-compensating the arches. That is establising relatively ideal inclination of the incisors and molars. This includes correction of the proclined upper incisors and retroclined lower incisors. It also includes getting the upper and lower posterior teeth uprighted and centered over the ridges. ᕤ Make the anterior and poste-rior crossbite worse to create space for the surgeon to have room to move the bones into anterior and posterior crossbite correction, respectively. Ironically, the orthodontics needed in a surgical case is easier than treating these cases without orthognathic surgery. A bigger chal-lenge is patient management of the case because: (Figs. 13-16) ᕡ Straightening the teeth ᕢ Banding/bonding all of the teeth to facilitate arch coordi-nation and to optimally level the curve-of-Spee. www.orthodontics.com Winter 2022 21
Journal of the American Orthodontic Society Winter 2022: Page 21