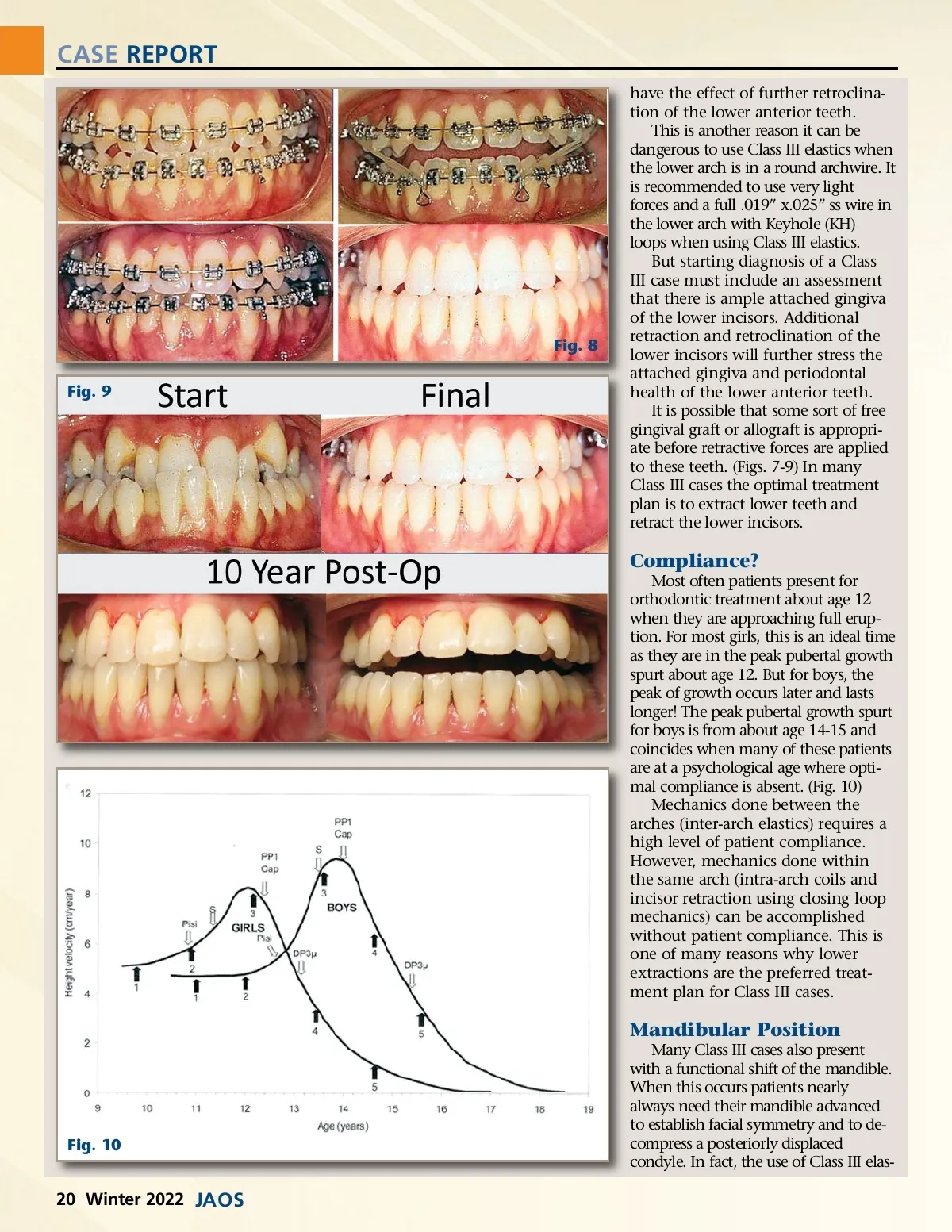
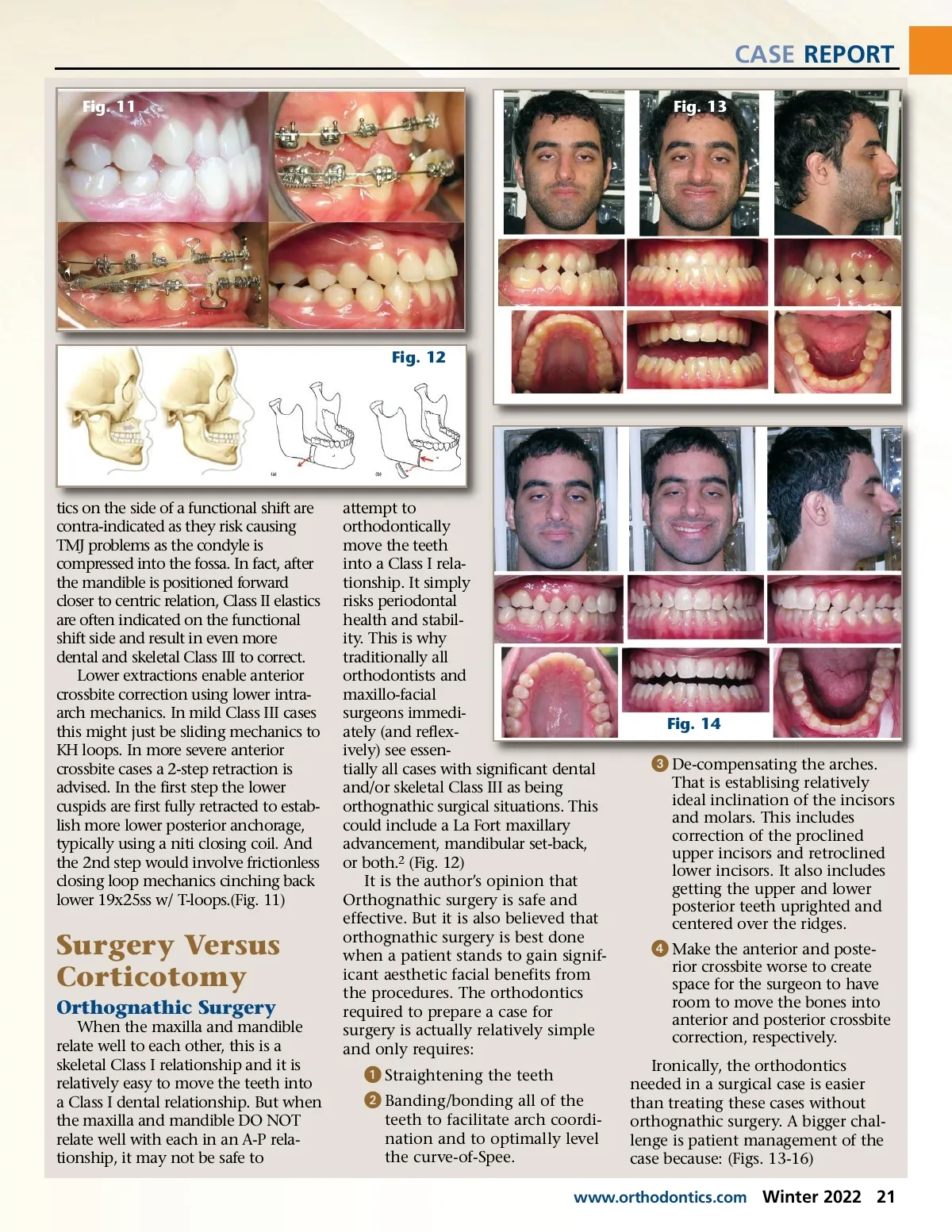
CASE REPORT have the effect of further retroclina-tion of the lower anterior teeth. This is another reason it can be dangerous to use Class III elastics when the lower arch is in a round archwire. It is recommended to use very light forces and a full .019” x.025” ss wire in the lower arch with Keyhole (KH) loops when using Class III elastics. But starting diagnosis of a Class III case must include an assessment that there is ample attached gingiva of the lower incisors. Additional retraction and retroclination of the lower incisors will further stress the attached gingiva and periodontal health of the lower anterior teeth. It is possible that some sort of free gingival graft or allograft is appropri-ate before retractive forces are applied to these teeth. (Figs. 7-9) In many Class III cases the optimal treatment plan is to extract lower teeth and retract the lower incisors. Fig. 8 Fig. 9 Compliance? Most often patients present for orthodontic treatment about age 12 when they are approaching full erup-tion. For most girls, this is an ideal time as they are in the peak pubertal growth spurt about age 12. But for boys, the peak of growth occurs later and lasts longer! The peak pubertal growth spurt for boys is from about age 14-15 and coincides when many of these patients are at a psychological age where opti-mal compliance is absent. (Fig. 10) Mechanics done between the arches (inter-arch elastics) requires a high level of patient compliance. However, mechanics done within the same arch (intra-arch coils and incisor retraction using closing loop mechanics) can be accomplished without patient compliance. This is one of many reasons why lower extractions are the preferred treat-ment plan for Class III cases. Mandibular Position Many Class III cases also present with a functional shift of the mandible. When this occurs patients nearly always need their mandible advanced to establish facial symmetry and to de-compress a posteriorly displaced condyle. In fact, the use of Class III elas-Fig. 10 20 Winter 2022 JAOS
Journal of the American Orthodontic Society Winter 2022: Page 20