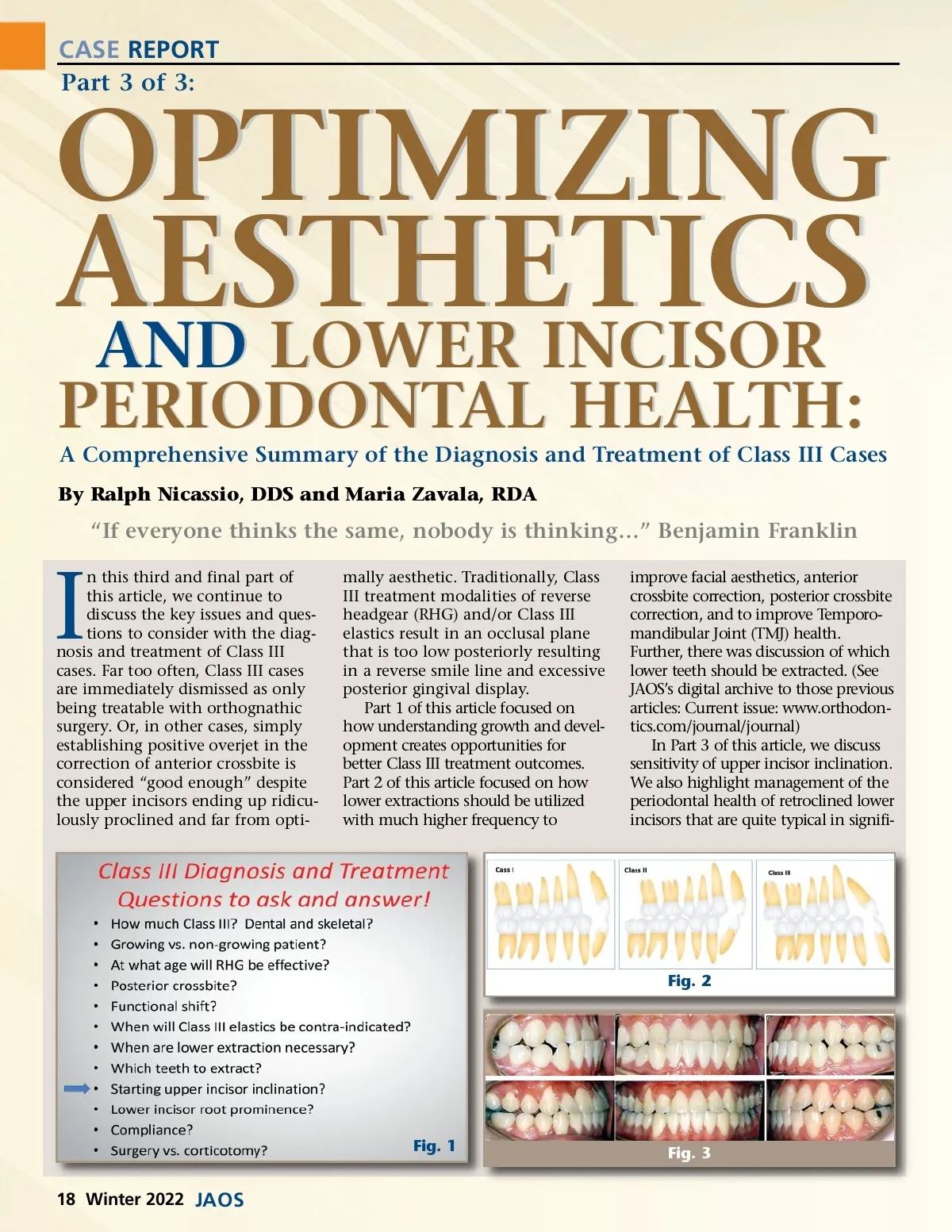
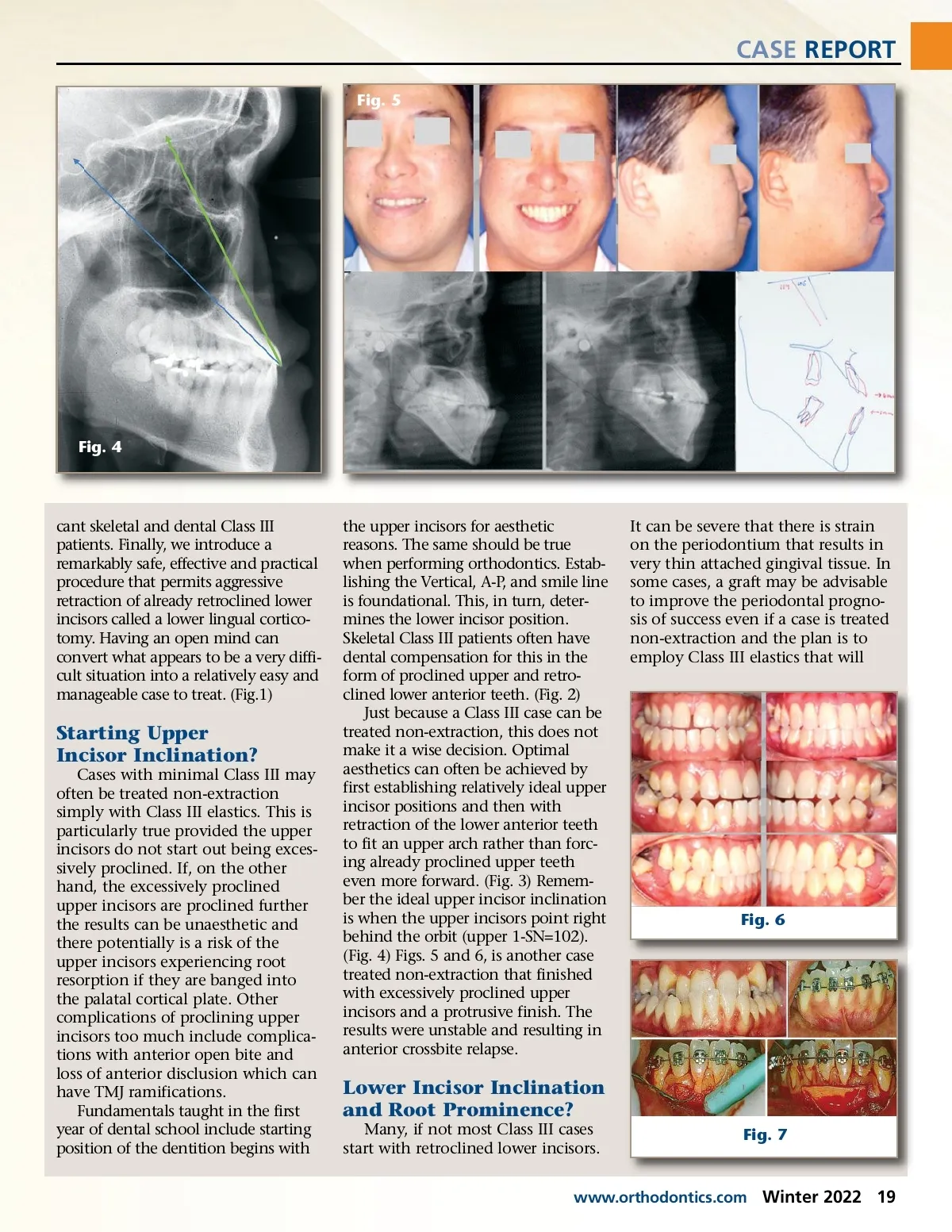
CASE REPORT Fig. 5 Fig. 4 cant skeletal and dental Class III patients. Finally, we introduce a remarkably safe, effective and practical procedure that permits aggressive retraction of already retroclined lower incisors called a lower lingual cortico-tomy. Having an open mind can convert what appears to be a very diffi-cult situation into a relatively easy and manageable case to treat. (Fig.1) Starting Upper Incisor Inclination? Cases with minimal Class III may often be treated non-extraction simply with Class III elastics. This is particularly true provided the upper incisors do not start out being exces-sively proclined. If, on the other hand, the excessively proclined upper incisors are proclined further the results can be unaesthetic and there potentially is a risk of the upper incisors experiencing root resorption if they are banged into the palatal cortical plate. Other complications of proclining upper incisors too much include complica-tions with anterior open bite and loss of anterior disclusion which can have TMJ ramifications. Fundamentals taught in the first year of dental school include starting position of the dentition begins with the upper incisors for aesthetic reasons. The same should be true when performing orthodontics. Estab-lishing the Vertical, A-P, and smile line is foundational. This, in turn, deter-mines the lower incisor position. Skeletal Class III patients often have dental compensation for this in the form of proclined upper and retro-clined lower anterior teeth. (Fig. 2) Just because a Class III case can be treated non-extraction, this does not make it a wise decision. Optimal aesthetics can often be achieved by first establishing relatively ideal upper incisor positions and then with retraction of the lower anterior teeth to fit an upper arch rather than forc-ing already proclined upper teeth even more forward. (Fig. 3) Remem-ber the ideal upper incisor inclination is when the upper incisors point right behind the orbit (upper 1-SN=102). (Fig. 4) Figs. 5 and 6, is another case treated non-extraction that finished with excessively proclined upper incisors and a protrusive finish. The results were unstable and resulting in anterior crossbite relapse. It can be severe that there is strain on the periodontium that results in very thin attached gingival tissue. In some cases, a graft may be advisable to improve the periodontal progno-sis of success even if a case is treated non-extraction and the plan is to employ Class III elastics that will Fig. 6 Lower Incisor Inclination and Root Prominence? Many, if not most Class III cases start with retroclined lower incisors. Fig. 7 www.orthodontics.com Winter 2022 19
Journal of the American Orthodontic Society Winter 2022: Page 19