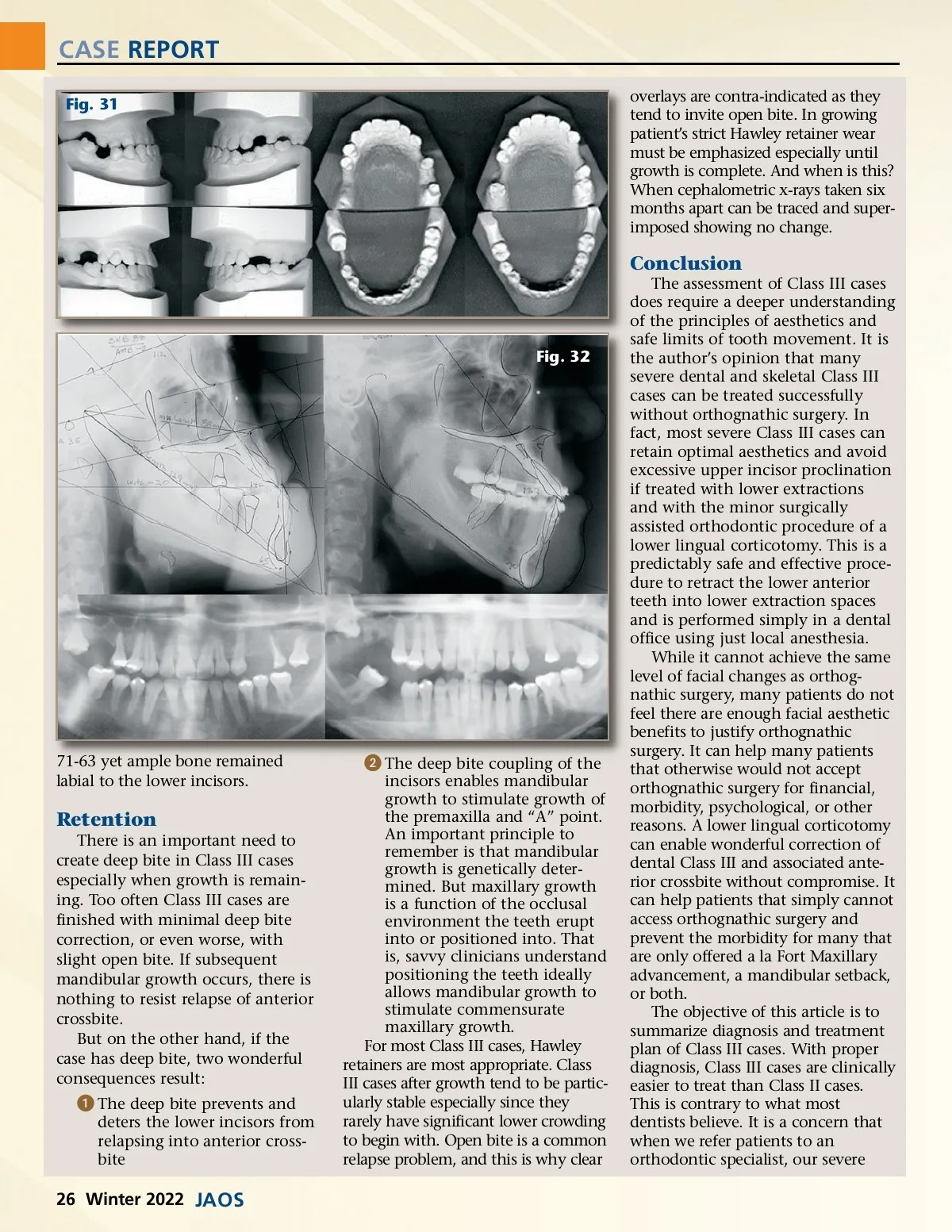
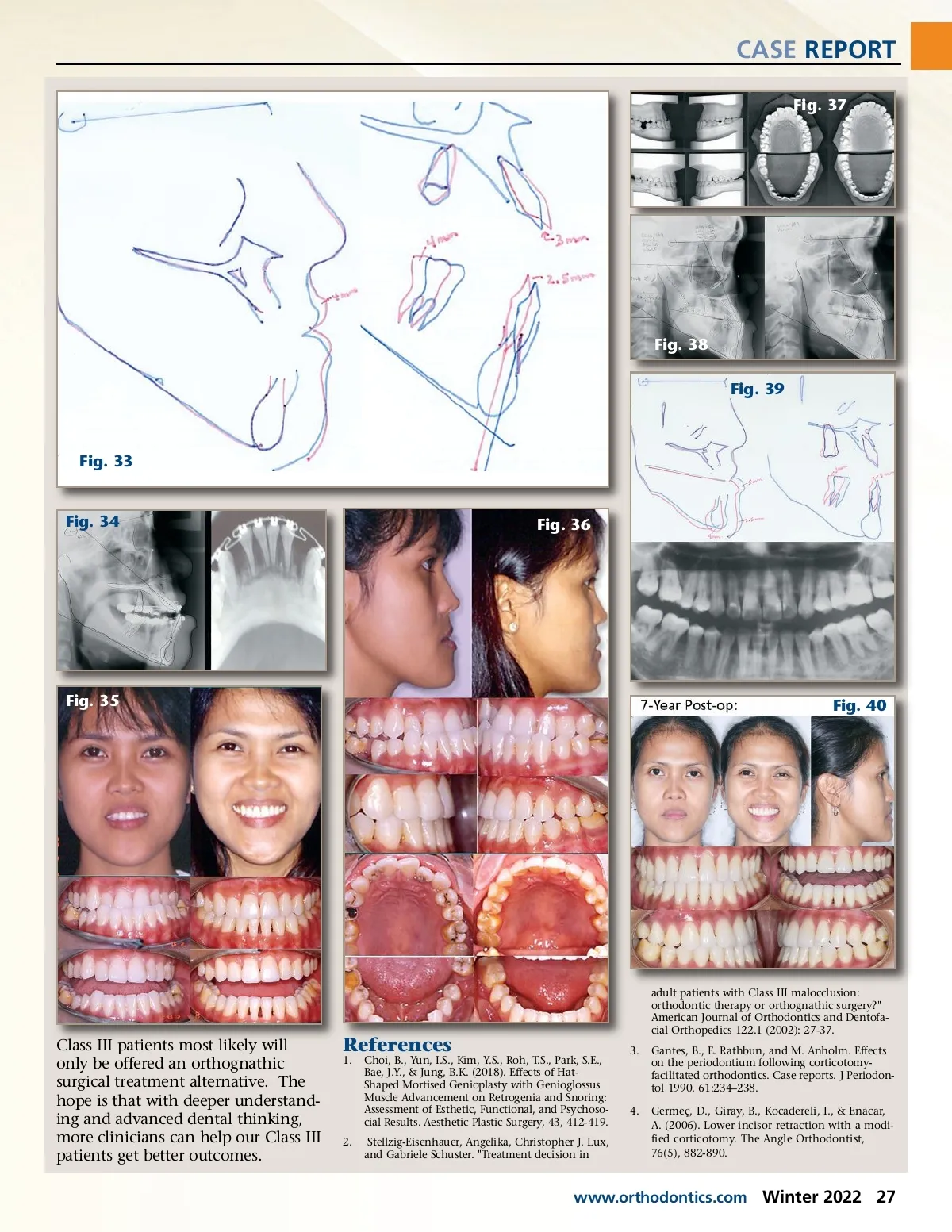
CASE REPORT Fig. 31 overlays are contra-indicated as they tend to invite open bite. In growing patient’s strict Hawley retainer wear must be emphasized especially until growth is complete. And when is this? When cephalometric x-rays taken six months apart can be traced and super-imposed showing no change. Conclusion The assessment of Class III cases does require a deeper understanding of the principles of aesthetics and safe limits of tooth movement. It is the author’s opinion that many severe dental and skeletal Class III cases can be treated successfully without orthognathic surgery. In fact, most severe Class III cases can retain optimal aesthetics and avoid excessive upper incisor proclination if treated with lower extractions and with the minor surgically assisted orthodontic procedure of a lower lingual corticotomy. This is a predictably safe and effective proce-dure to retract the lower anterior teeth into lower extraction spaces and is performed simply in a dental office using just local anesthesia. While it cannot achieve the same level of facial changes as orthog-nathic surgery, many patients do not feel there are enough facial aesthetic benefits to justify orthognathic surgery. It can help many patients that otherwise would not accept orthognathic surgery for financial, morbidity, psychological, or other reasons. A lower lingual corticotomy can enable wonderful correction of dental Class III and associated ante-rior crossbite without compromise. It can help patients that simply cannot access orthognathic surgery and prevent the morbidity for many that are only offered a la Fort Maxillary advancement, a mandibular setback, or both. The objective of this article is to summarize diagnosis and treatment plan of Class III cases. With proper diagnosis, Class III cases are clinically easier to treat than Class II cases. This is contrary to what most dentists believe. It is a concern that when we refer patients to an orthodontic specialist, our severe Fig. 32 71-63 yet ample bone remained labial to the lower incisors. ᕢ The deep bite coupling of the incisors enables mandibular growth to stimulate growth of the premaxilla and “A” point. An important principle to remember is that mandibular growth is genetically deter-mined. But maxillary growth is a function of the occlusal environment the teeth erupt into or positioned into. That is, savvy clinicians understand positioning the teeth ideally allows mandibular growth to stimulate commensurate maxillary growth. For most Class III cases, Hawley retainers are most appropriate. Class III cases after growth tend to be partic-ularly stable especially since they rarely have significant lower crowding to begin with. Open bite is a common relapse problem, and this is why clear Retention There is an important need to create deep bite in Class III cases especially when growth is remain-ing. Too often Class III cases are finished with minimal deep bite correction, or even worse, with slight open bite. If subsequent mandibular growth occurs, there is nothing to resist relapse of anterior crossbite. But on the other hand, if the case has deep bite, two wonderful consequences result: ᕡ The deep bite prevents and deters the lower incisors from relapsing into anterior cross-bite 26 Winter 2022 JAOS
Journal of the American Orthodontic Society Winter 2022: Page 26