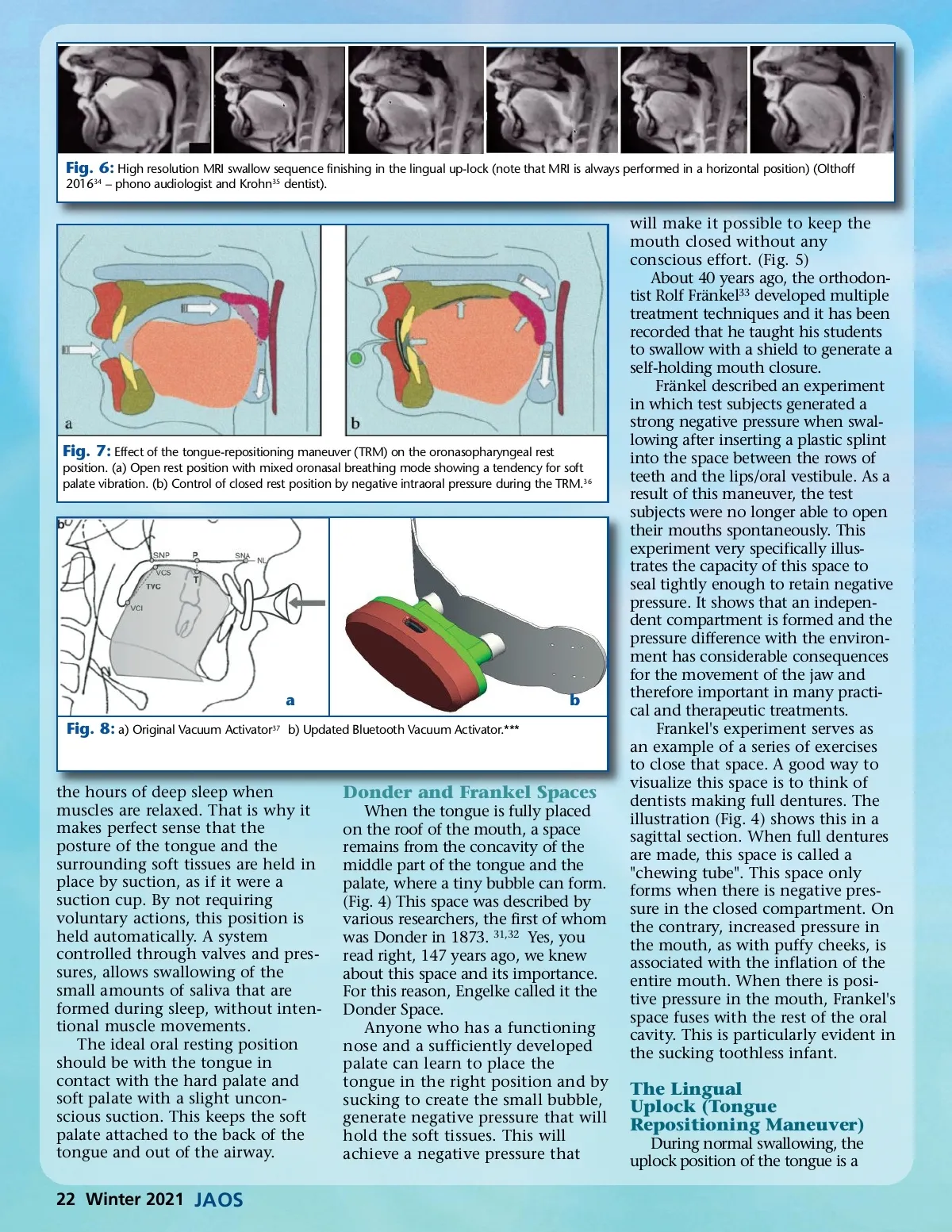
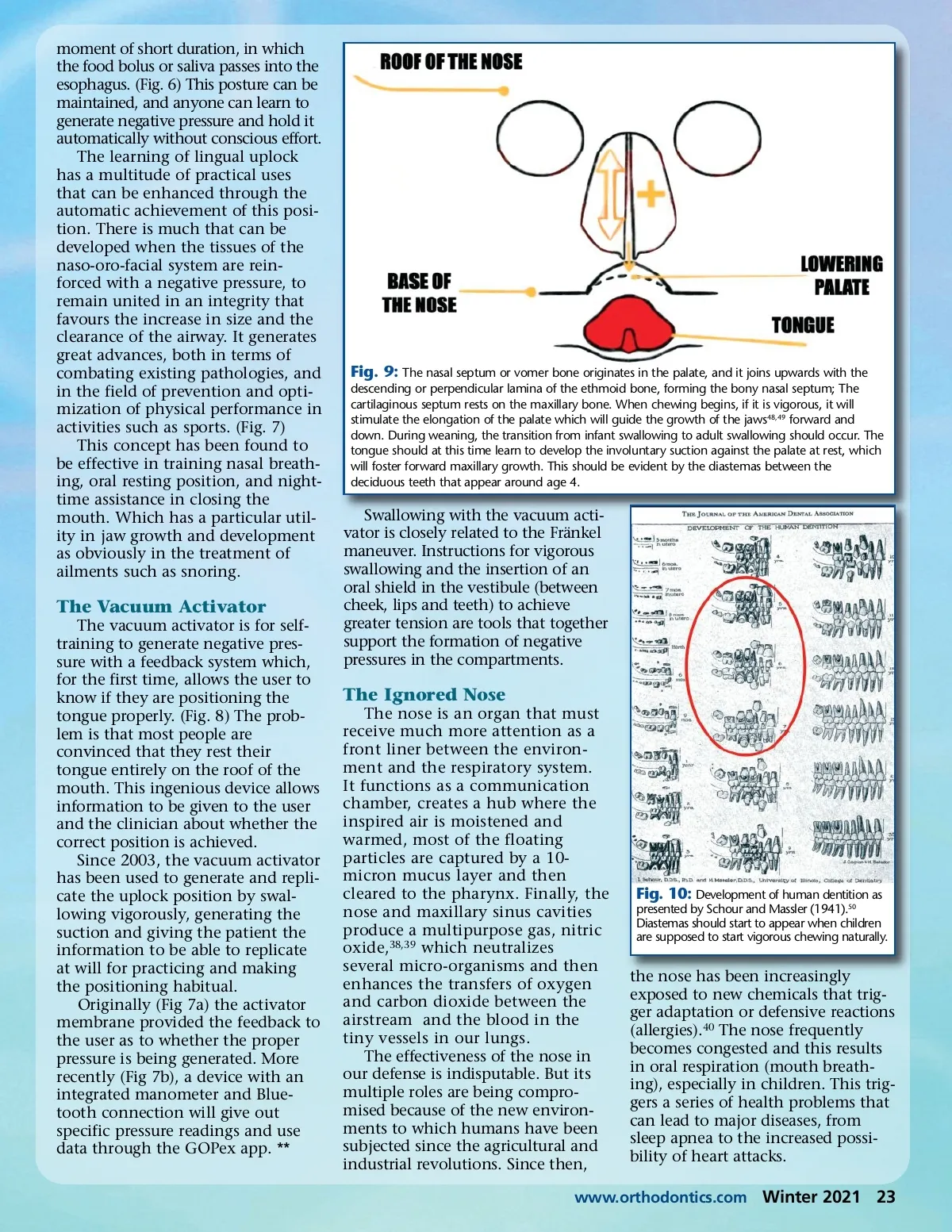
Fig. 6: High resolution MRI swallow sequence finishing in the lingual up-lock (note that MRI is always performed in a horizontal position) (Olthoff 2016 34 – phono audiologist and Krohn 35 dentist). Fig. 7: Effect of the tongue-repositioning maneuver (TRM) on the oronasopharyngeal rest position. (a) Open rest position with mixed oronasal breathing mode showing a tendency for soft palate vibration. (b) Control of closed rest position by negative intraoral pressure during the TRM. 36 ab Fig. 8: a) Original Vacuum Activator 37 b) Updated Bluetooth Vacuum Activator.*** the hours of deep sleep when muscles are relaxed. That is why it makes perfect sense that the posture of the tongue and the surrounding soft tissues are held in place by suction, as if it were a suction cup. By not requiring voluntary actions, this position is held automatically. A system controlled through valves and pres-sures, allows swallowing of the small amounts of saliva that are formed during sleep, without inten-tional muscle movements. The ideal oral resting position should be with the tongue in contact with the hard palate and soft palate with a slight uncon-scious suction. This keeps the soft palate attached to the back of the tongue and out of the airway. Donder and Frankel Spaces When the tongue is fully placed on the roof of the mouth, a space remains from the concavity of the middle part of the tongue and the palate, where a tiny bubble can form. (Fig. 4) This space was described by various researchers, the first of whom was Donder in 1873. 31,32 Yes, you read right, 147 years ago, we knew about this space and its importance. For this reason, Engelke called it the Donder Space. Anyone who has a functioning nose and a sufficiently developed palate can learn to place the tongue in the right position and by sucking to create the small bubble, generate negative pressure that will hold the soft tissues. This will achieve a negative pressure that will make it possible to keep the mouth closed without any conscious effort. (Fig. 5) About 40 years ago, the orthodon-tist Rolf Fränkel 33 developed multiple treatment techniques and it has been recorded that he taught his students to swallow with a shield to generate a self-holding mouth closure. Fränkel described an experiment in which test subjects generated a strong negative pressure when swal-lowing after inserting a plastic splint into the space between the rows of teeth and the lips/oral vestibule. As a result of this maneuver, the test subjects were no longer able to open their mouths spontaneously. This experiment very specifically illus-trates the capacity of this space to seal tightly enough to retain negative pressure. It shows that an indepen-dent compartment is formed and the pressure difference with the environ-ment has considerable consequences for the movement of the jaw and therefore important in many practi-cal and therapeutic treatments. Frankel's experiment serves as an example of a series of exercises to close that space. A good way to visualize this space is to think of dentists making full dentures. The illustration (Fig. 4) shows this in a sagittal section. When full dentures are made, this space is called a "chewing tube". This space only forms when there is negative pres-sure in the closed compartment. On the contrary, increased pressure in the mouth, as with puffy cheeks, is associated with the inflation of the entire mouth. When there is posi-tive pressure in the mouth, Frankel's space fuses with the rest of the oral cavity. This is particularly evident in the sucking toothless infant. The Lingual Uplock (Tongue Repositioning Maneuver) During normal swallowing, the uplock position of the tongue is a 22 Winter 2021 JAOS
Journal of the American Orthodontic Society Winter 2021: Page 22