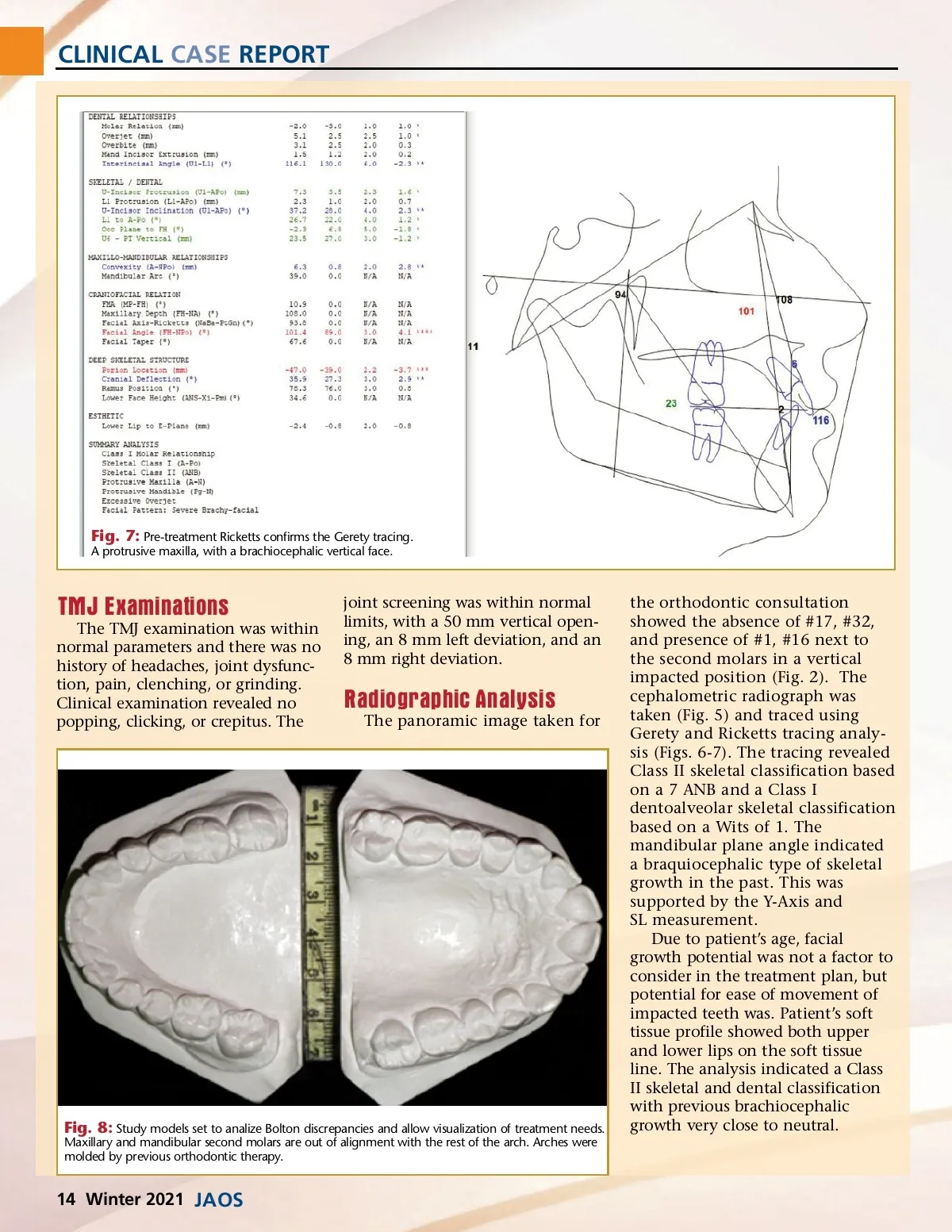
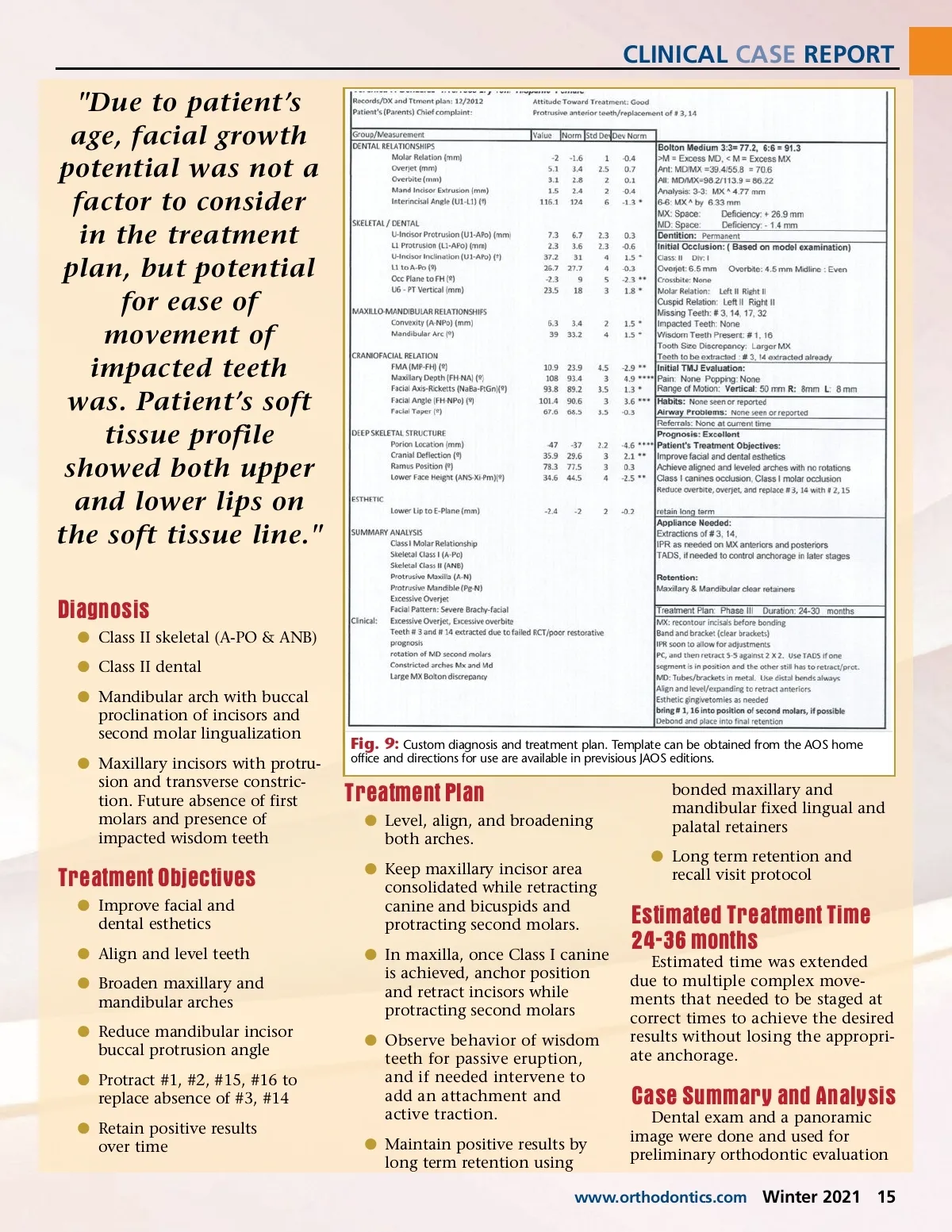
CLINICAL CASE REPORT Fig. 7: Pre-treatment Ricketts confirms the Gerety tracing. A protrusive maxilla, with a brachiocephalic vertical face. TMJ Examinations The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunc-tion, pain, clenching, or grinding. Clinical examination revealed no popping, clicking, or crepitus. The joint screening was within normal limits, with a 50 mm vertical open-ing, an 8 mm left deviation, and an 8 mm right deviation. Radiographic Analysis The panoramic image taken for Fig. 8: Study models set to analize Bolton discrepancies and allow visualization of treatment needs. Maxillary and mandibular second molars are out of alignment with the rest of the arch. Arches were molded by previous orthodontic therapy. the orthodontic consultation showed the absence of #17, #32, and presence of #1, #16 next to the second molars in a vertical impacted position (Fig. 2). The cephalometric radiograph was taken (Fig. 5) and traced using Gerety and Ricketts tracing analy-sis (Figs. 6-7). The tracing revealed Class II skeletal classification based on a 7 ANB and a Class I dentoalveolar skeletal classification based on a Wits of 1. The mandibular plane angle indicated a braquiocephalic type of skeletal growth in the past. This was supported by the Y-Axis and SL measurement. Due to patient’s age, facial growth potential was not a factor to consider in the treatment plan, but potential for ease of movement of impacted teeth was. Patient’s soft tissue profile showed both upper and lower lips on the soft tissue line. The analysis indicated a Class II skeletal and dental classification with previous brachiocephalic growth very close to neutral. 14 Winter 2021 JAOS
Journal of the American Orthodontic Society Winter 2021: Page 14