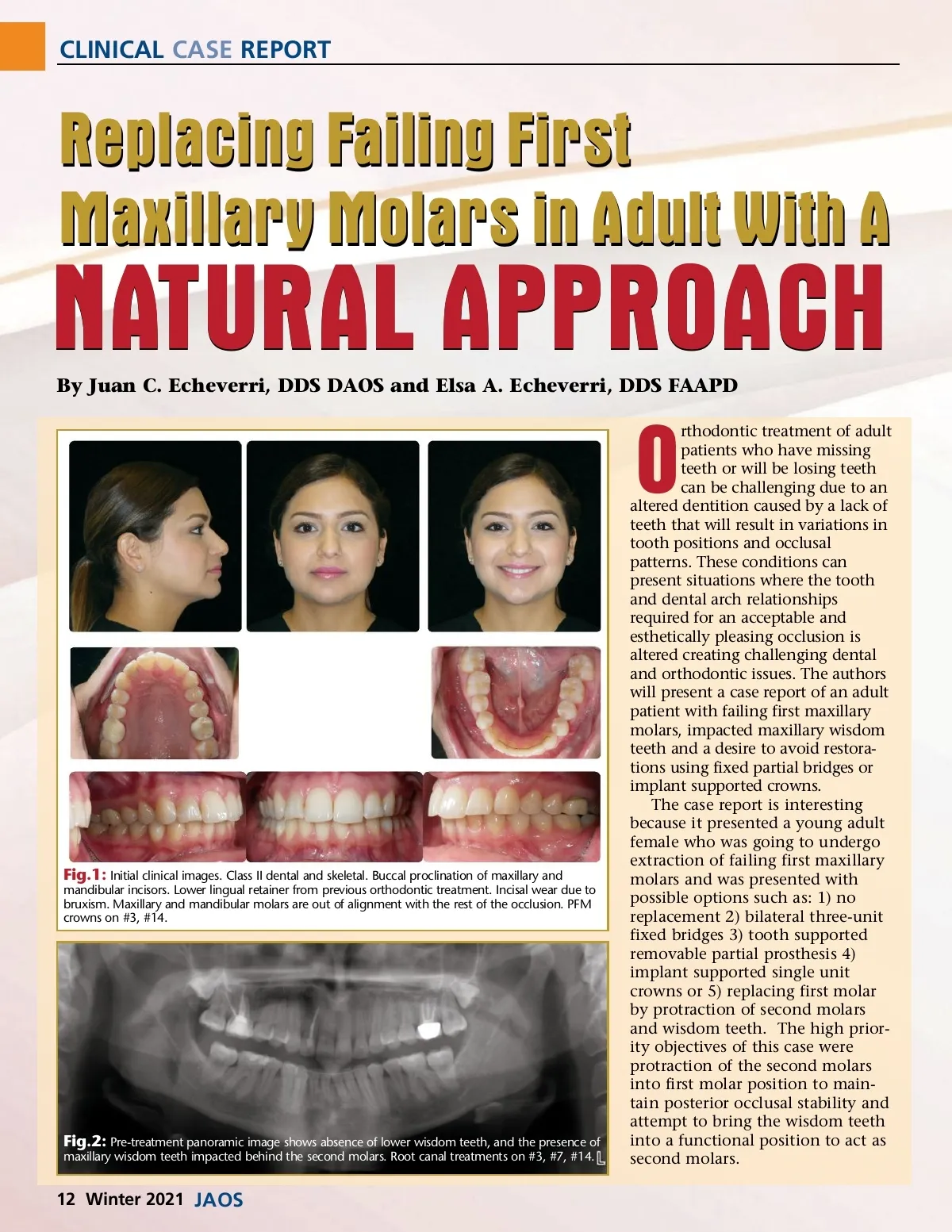
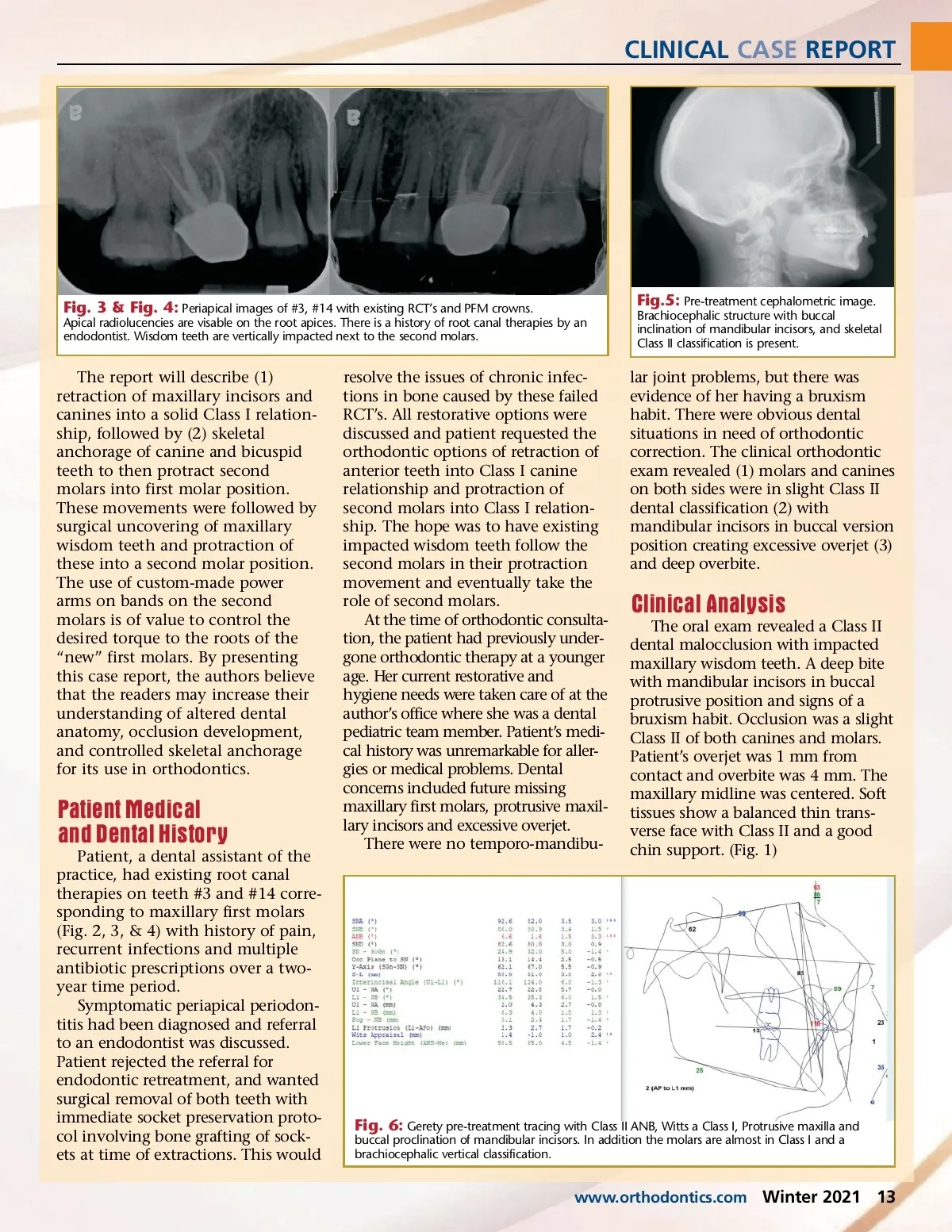
CLINICAL CASE REPORT Fig. 3 & Fig. 4: Periapical images of #3, #14 with existing RCT’s and PFM crowns. Apical radiolucencies are visable on the root apices. There is a history of root canal therapies by an endodontist. Wisdom teeth are vertically impacted next to the second molars. Fig.5: Pre-treatment cephalometric image. Brachiocephalic structure with buccal inclination of mandibular incisors, and skeletal Class II classification is present. The report will describe (1) retraction of maxillary incisors and canines into a solid Class I relation-ship, followed by (2) skeletal anchorage of canine and bicuspid teeth to then protract second molars into first molar position. These movements were followed by surgical uncovering of maxillary wisdom teeth and protraction of these into a second molar position. The use of custom-made power arms on bands on the second molars is of value to control the desired torque to the roots of the “new” first molars. By presenting this case report, the authors believe that the readers may increase their understanding of altered dental anatomy, occlusion development, and controlled skeletal anchorage for its use in orthodontics. Patient Medical and Dental History Patient, a dental assistant of the practice, had existing root canal therapies on teeth #3 and #14 corre-sponding to maxillary first molars (Fig. 2, 3, & 4) with history of pain, recurrent infections and multiple antibiotic prescriptions over a two-year time period. Symptomatic periapical periodon-titis had been diagnosed and referral to an endodontist was discussed. Patient rejected the referral for endodontic retreatment, and wanted surgical removal of both teeth with immediate socket preservation proto-col involving bone grafting of sock-ets at time of extractions. This would resolve the issues of chronic infec-tions in bone caused by these failed RCT’s. All restorative options were discussed and patient requested the orthodontic options of retraction of anterior teeth into Class I canine relationship and protraction of second molars into Class I relation-ship. The hope was to have existing impacted wisdom teeth follow the second molars in their protraction movement and eventually take the role of second molars. At the time of orthodontic consulta-tion, the patient had previously under-gone orthodontic therapy at a younger age. Her current restorative and hygiene needs were taken care of at the author’s office where she was a dental pediatric team member. Patient’s medi-cal history was unremarkable for aller-gies or medical problems. Dental concerns included future missing maxillary first molars, protrusive maxil-lary incisors and excessive overjet. There were no temporo-mandibu-lar joint problems, but there was evidence of her having a bruxism habit. There were obvious dental situations in need of orthodontic correction. The clinical orthodontic exam revealed (1) molars and canines on both sides were in slight Class II dental classification (2) with mandibular incisors in buccal version position creating excessive overjet (3) and deep overbite. Clinical Analysis The oral exam revealed a Class II dental malocclusion with impacted maxillary wisdom teeth. A deep bite with mandibular incisors in buccal protrusive position and signs of a bruxism habit. Occlusion was a slight Class II of both canines and molars. Patient’s overjet was 1 mm from contact and overbite was 4 mm. The maxillary midline was centered. Soft tissues show a balanced thin trans-verse face with Class II and a good chin support. (Fig. 1) Fig. 6: Gerety pre-treatment tracing with Class II ANB, Witts a Class I, Protrusive maxilla and buccal proclination of mandibular incisors. In addition the molars are almost in Class I and a brachiocephalic vertical classification. www.orthodontics.com Winter 2021 13
Journal of the American Orthodontic Society Winter 2021: Page 13