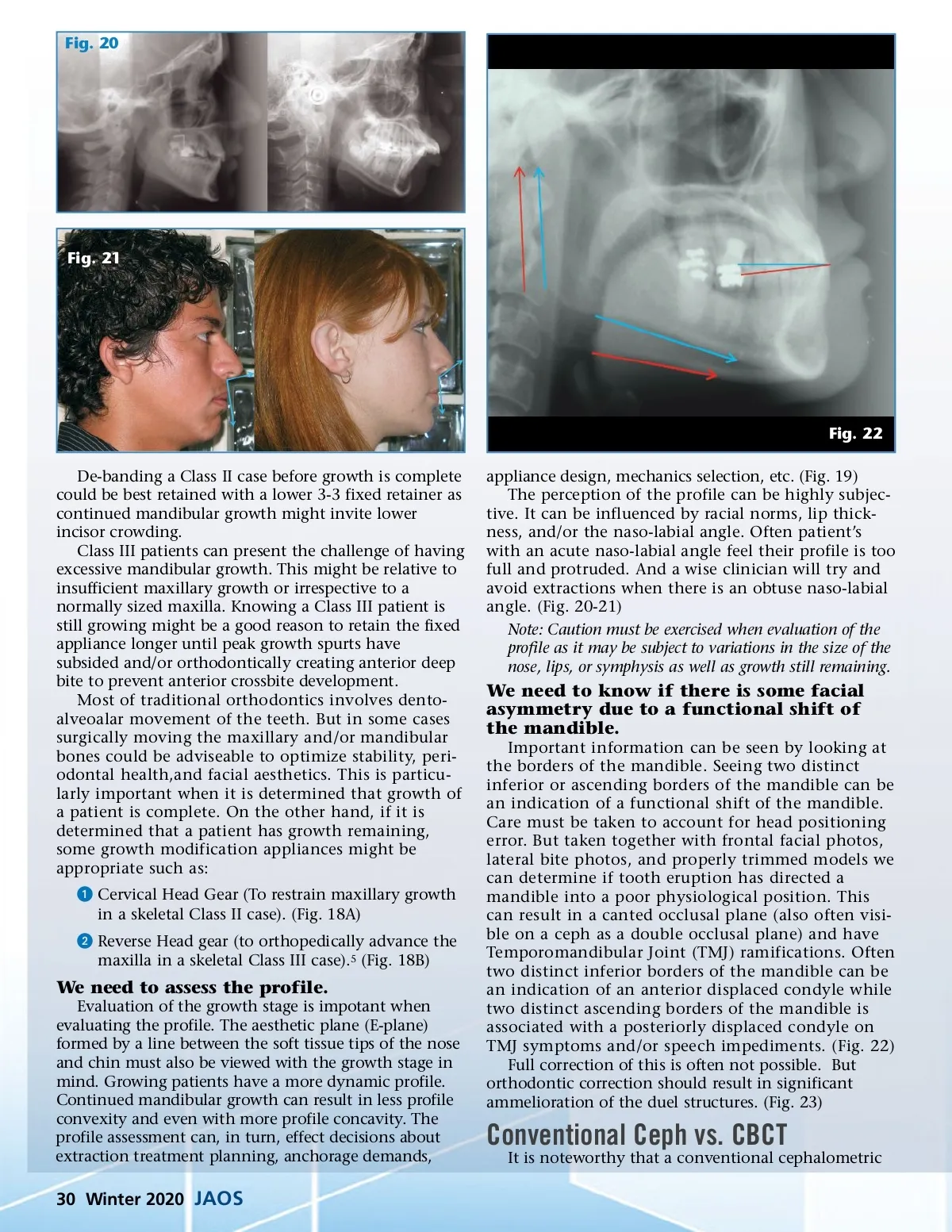
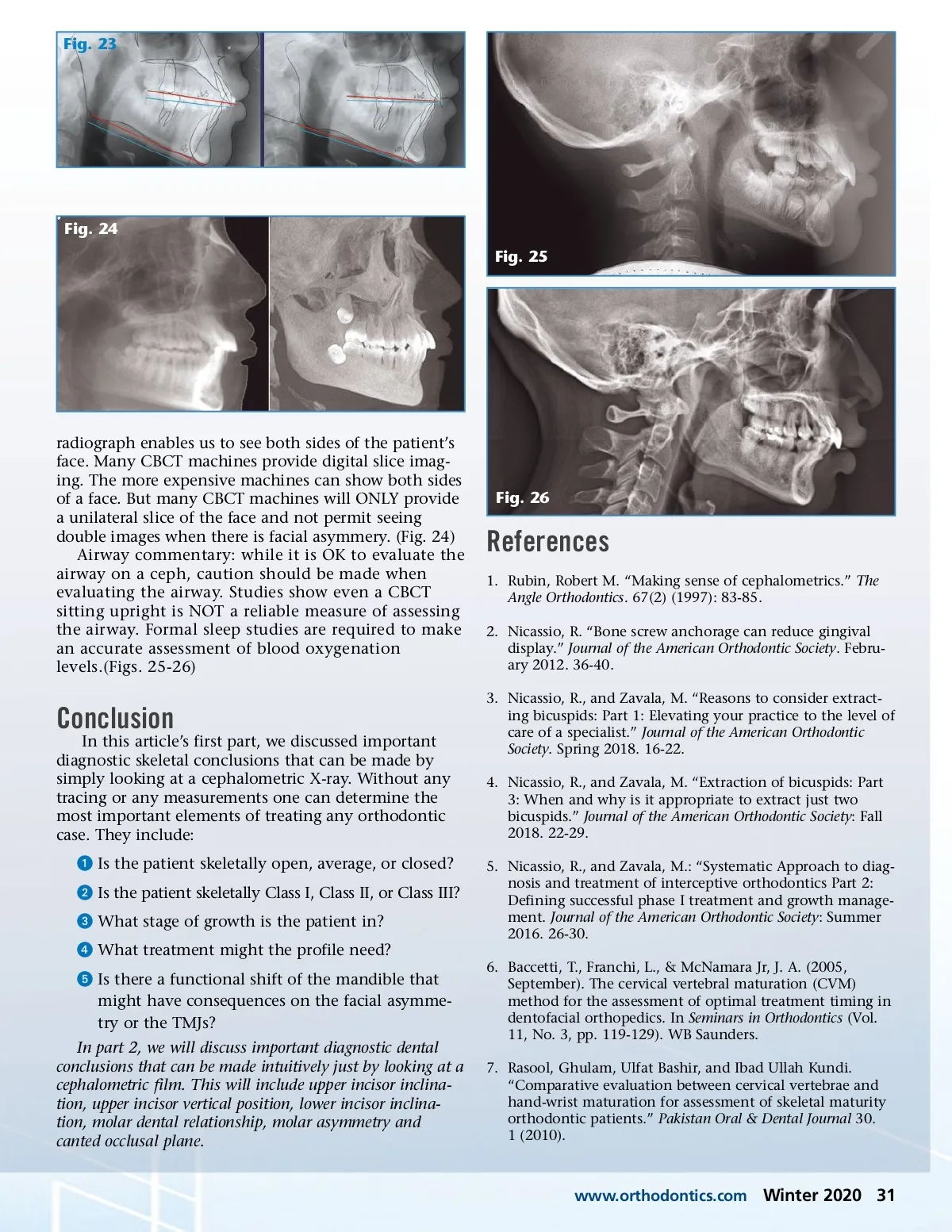
Fig. 20 Fig. 21 Fig. 22 De-banding a Class II case before growth is complete could be best retained with a lower 3-3 fixed retainer as continued mandibular growth might invite lower incisor crowding. Class III patients can present the challenge of having excessive mandibular growth. This might be relative to insufficient maxillary growth or irrespective to a normally sized maxilla. Knowing a Class III patient is still growing might be a good reason to retain the fixed appliance longer until peak growth spurts have subsided and/or orthodontically creating anterior deep bite to prevent anterior crossbite development. Most of traditional orthodontics involves dento-alveoalar movement of the teeth. But in some cases surgically moving the maxillary and/or mandibular bones could be adviseable to optimize stability, peri-odontal health,and facial aesthetics. This is particu-larly important when it is determined that growth of a patient is complete. On the other hand, if it is determined that a patient has growth remaining, some growth modification appliances might be appropriate such as: ᕡ Cervical Head Gear (To restrain maxillary growth in a skeletal Class II case). (Fig. 18A) ᕢ Reverse Head gear (to orthopedically advance the maxilla in a skeletal Class III case). 5 (Fig. 18B) appliance design, mechanics selection, etc. (Fig. 19) The perception of the profile can be highly subjec-tive. It can be influenced by racial norms, lip thick-ness, and/or the naso-labial angle. Often patient’s with an acute naso-labial angle feel their profile is too full and protruded. And a wise clinician will try and avoid extractions when there is an obtuse naso-labial angle. (Fig. 20-21) Note: Caution must be exercised when evaluation of the profile as it may be subject to variations in the size of the nose, lips, or symphysis as well as growth still remaining. We need to know if there is some facial asymmetry due to a functional shift of the mandible. Important information can be seen by looking at the borders of the mandible. Seeing two distinct inferior or ascending borders of the mandible can be an indication of a functional shift of the mandible. Care must be taken to account for head positioning error. But taken together with frontal facial photos, lateral bite photos, and properly trimmed models we can determine if tooth eruption has directed a mandible into a poor physiological position. This can result in a canted occlusal plane (also often visi-ble on a ceph as a double occlusal plane) and have Temporomandibular Joint (TMJ) ramifications. Often two distinct inferior borders of the mandible can be an indication of an anterior displaced condyle while two distinct ascending borders of the mandible is associated with a posteriorly displaced condyle on TMJ symptoms and/or speech impediments. (Fig. 22) Full correction of this is often not possible. But orthodontic correction should result in significant ammelioration of the duel structures. (Fig. 23) We need to assess the profile. Evaluation of the growth stage is impotant when evaluating the profile. The aesthetic plane (E-plane) formed by a line between the soft tissue tips of the nose and chin must also be viewed with the growth stage in mind. Growing patients have a more dynamic profile. Continued mandibular growth can result in less profile convexity and even with more profile concavity. The profile assessment can, in turn, effect decisions about extraction treatment planning, anchorage demands, Conventional Ceph vs. CBCT It is noteworthy that a conventional cephalometric 30 Winter 2020 JAOS
Journal of the American Orthodontic Society Winter 2020: Page 30