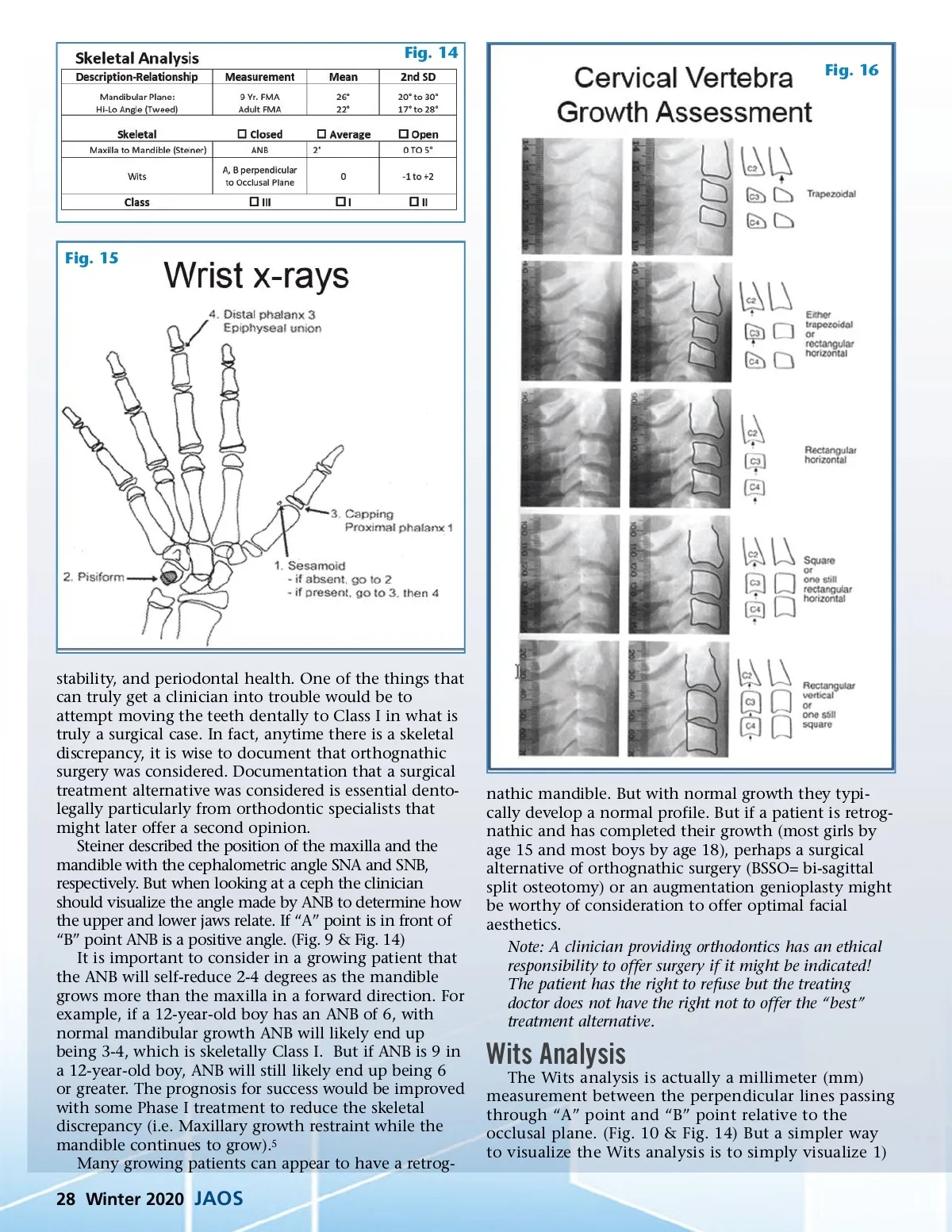
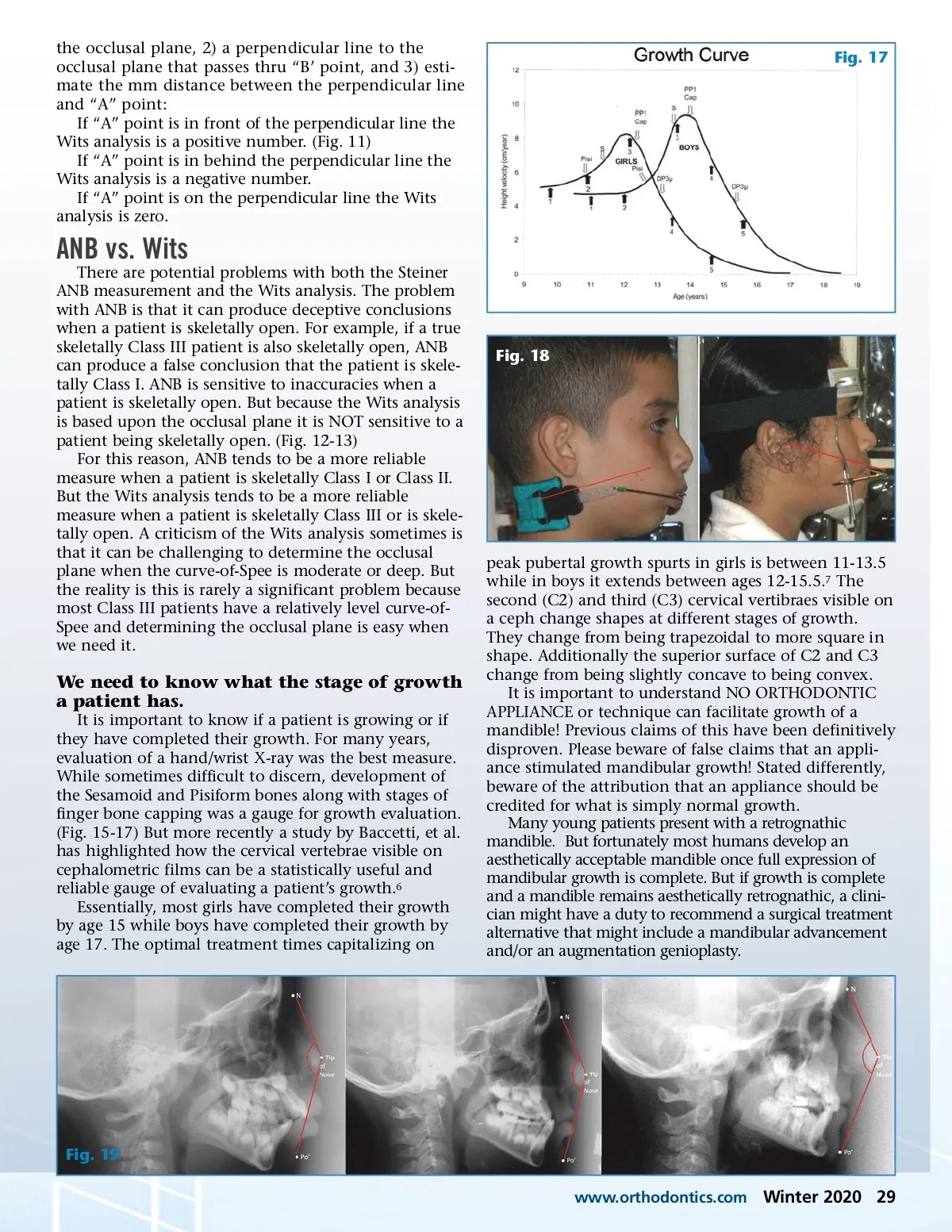
the occlusal plane, 2) a perpendicular line to the occlusal plane that passes thru “B’ point, and 3) esti-mate the mm distance between the perpendicular line and “A” point: If “A” point is in front of the perpendicular line the Wits analysis is a positive number. (Fig. 11) If “A” point is in behind the perpendicular line the Wits analysis is a negative number. If “A” point is on the perpendicular line the Wits analysis is zero. Fig. 17 ANB vs. Wits There are potential problems with both the Steiner ANB measurement and the Wits analysis. The problem with ANB is that it can produce deceptive conclusions when a patient is skeletally open. For example, if a true skeletally Class III patient is also skeletally open, ANB can produce a false conclusion that the patient is skele-tally Class I. ANB is sensitive to inaccuracies when a patient is skeletally open. But because the Wits analysis is based upon the occlusal plane it is NOT sensitive to a patient being skeletally open. (Fig. 12-13) For this reason, ANB tends to be a more reliable measure when a patient is skeletally Class I or Class II. But the Wits analysis tends to be a more reliable measure when a patient is skeletally Class III or is skele-tally open. A criticism of the Wits analysis sometimes is that it can be challenging to determine the occlusal plane when the curve-of-Spee is moderate or deep. But the reality is this is rarely a significant problem because most Class III patients have a relatively level curve-of-Spee and determining the occlusal plane is easy when we need it. Fig. 18 We need to know what the stage of growth a patient has. It is important to know if a patient is growing or if they have completed their growth. For many years, evaluation of a hand/wrist X-ray was the best measure. While sometimes difficult to discern, development of the Sesamoid and Pisiform bones along with stages of finger bone capping was a gauge for growth evaluation. (Fig. 15-17) But more recently a study by Baccetti, et al. has highlighted how the cervical vertebrae visible on cephalometric films can be a statistically useful and reliable gauge of evaluating a patient’s growth. 6 Essentially, most girls have completed their growth by age 15 while boys have completed their growth by age 17. The optimal treatment times capitalizing on peak pubertal growth spurts in girls is between 11-13.5 while in boys it extends between ages 12-15.5. 7 The second (C2) and third (C3) cervical vertibraes visible on a ceph change shapes at different stages of growth. They change from being trapezoidal to more square in shape. Additionally the superior surface of C2 and C3 change from being slightly concave to being convex. It is important to understand NO ORTHODONTIC APPLIANCE or technique can facilitate growth of a mandible! Previous claims of this have been definitively disproven. Please beware of false claims that an appli-ance stimulated mandibular growth! Stated differently, beware of the attribution that an appliance should be credited for what is simply normal growth. Many young patients present with a retrognathic mandible. But fortunately most humans develop an aesthetically acceptable mandible once full expression of mandibular growth is complete. But if growth is complete and a mandible remains aesthetically retrognathic, a clini-cian might have a duty to recommend a surgical treatment alternative that might include a mandibular advancement and/or an augmentation genioplasty. Fig. 19 www.orthodontics.com Winter 2020 29
Journal of the American Orthodontic Society Winter 2020: Page 29