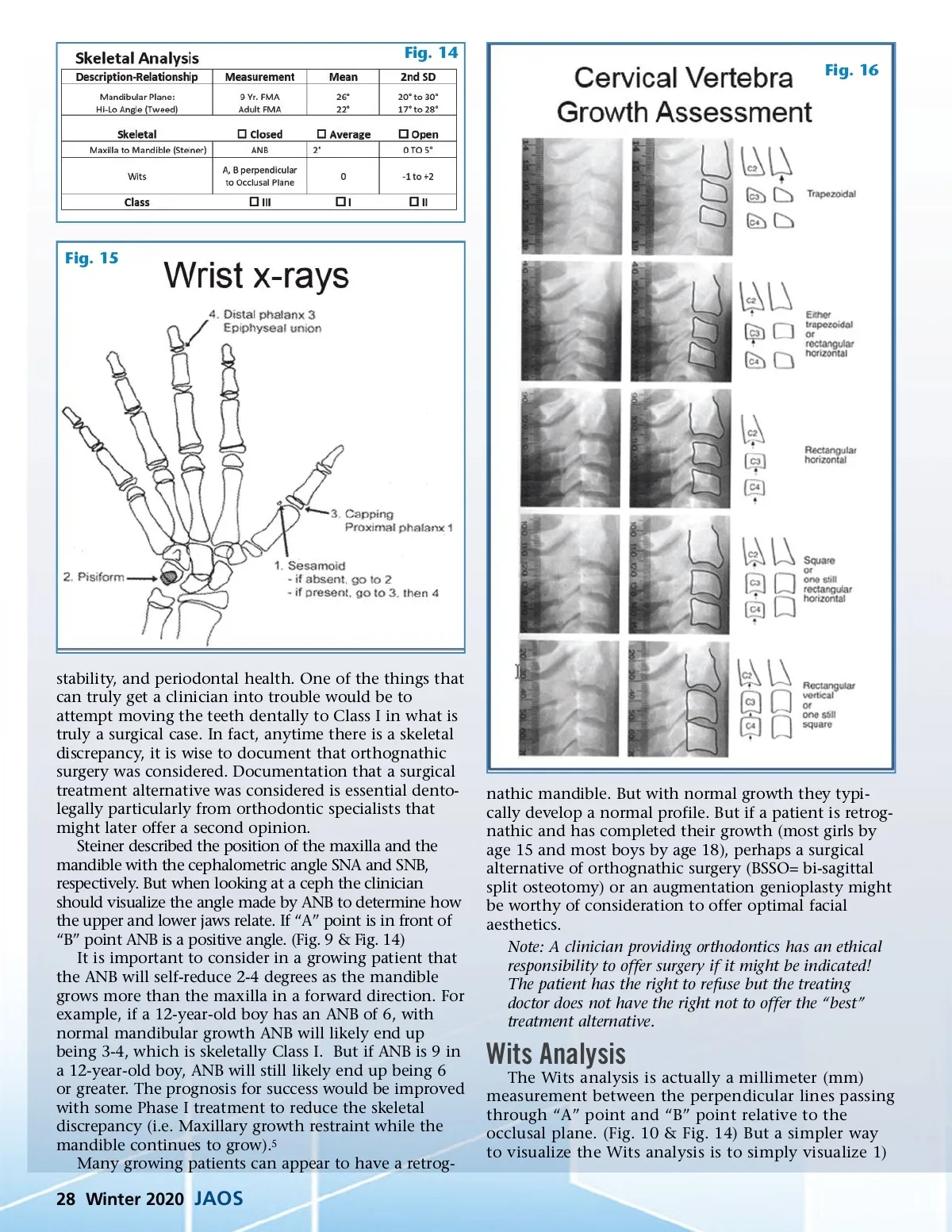
Fig. 14 Fig. 16 Fig. 15 stability, and periodontal health. One of the things that can truly get a clinician into trouble would be to attempt moving the teeth dentally to Class I in what is truly a surgical case. In fact, anytime there is a skeletal discrepancy, it is wise to document that orthognathic surgery was considered. Documentation that a surgical treatment alternative was considered is essential dento-legally particularly from orthodontic specialists that might later offer a second opinion. Steiner described the position of the maxilla and the mandible with the cephalometric angle SNA and SNB, respectively. But when looking at a ceph the clinician should visualize the angle made by ANB to determine how the upper and lower jaws relate. If “A” point is in front of “B” point ANB is a positive angle. (Fig. 9 & Fig. 14) It is important to consider in a growing patient that the ANB will self-reduce 2-4 degrees as the mandible grows more than the maxilla in a forward direction. For example, if a 12-year-old boy has an ANB of 6, with normal mandibular growth ANB will likely end up being 3-4, which is skeletally Class I. But if ANB is 9 in a 12-year-old boy, ANB will still likely end up being 6 or greater. The prognosis for success would be improved with some Phase I treatment to reduce the skeletal discrepancy (i.e. Maxillary growth restraint while the mandible continues to grow). 5 Many growing patients can appear to have a retrog-nathic mandible. But with normal growth they typi-cally develop a normal profile. But if a patient is retrog-nathic and has completed their growth (most girls by age 15 and most boys by age 18), perhaps a surgical alternative of orthognathic surgery (BSSO= bi-sagittal split osteotomy) or an augmentation genioplasty might be worthy of consideration to offer optimal facial aesthetics. Note: A clinician providing orthodontics has an ethical responsibility to offer surgery if it might be indicated! The patient has the right to refuse but the treating doctor does not have the right not to offer the “best” treatment alternative. Wits Analysis The Wits analysis is actually a millimeter (mm) measurement between the perpendicular lines passing through “A” point and “B” point relative to the occlusal plane. (Fig. 10 & Fig. 14) But a simpler way to visualize the Wits analysis is to simply visualize 1) 28 Winter 2020 JAOS
Journal of the American Orthodontic Society Winter 2020: Page 28