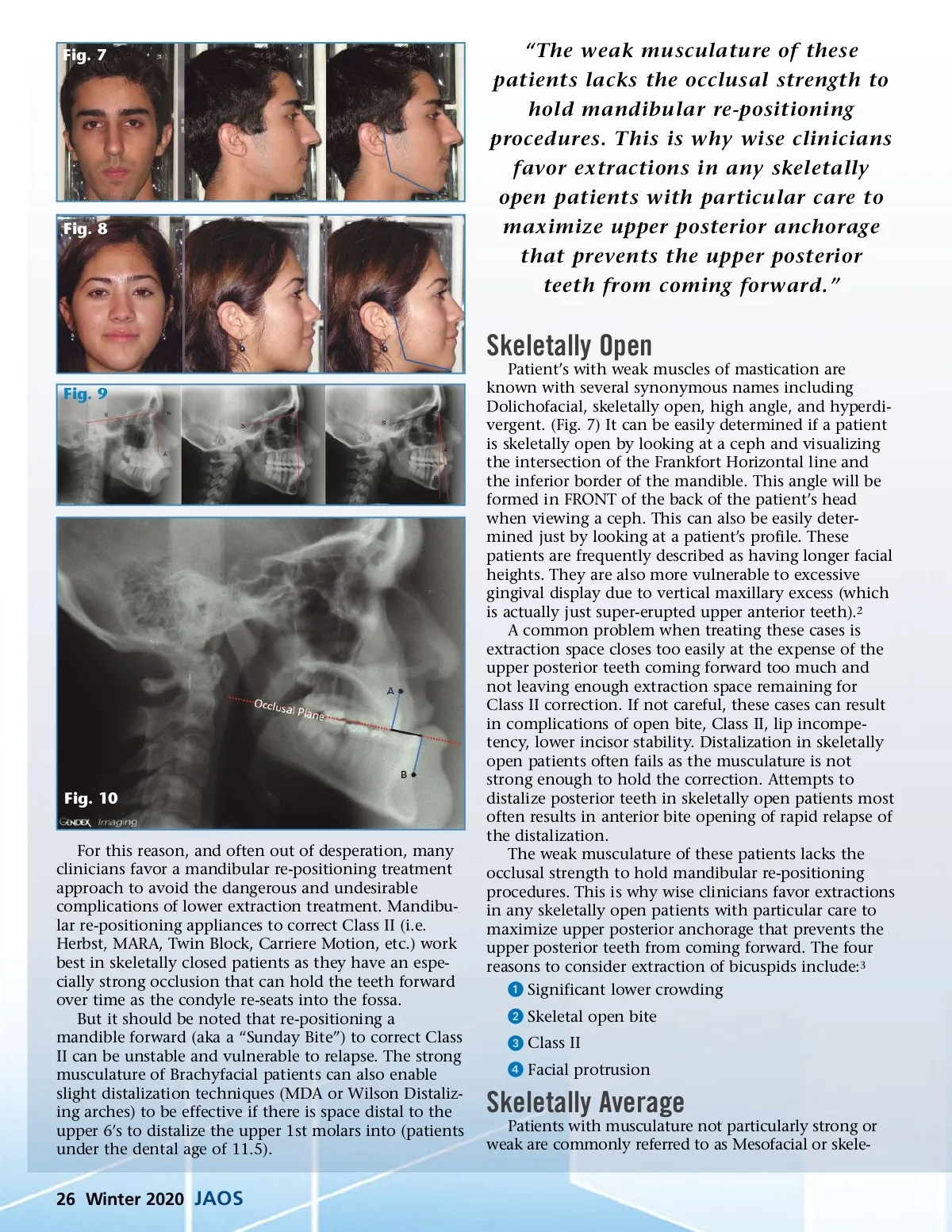
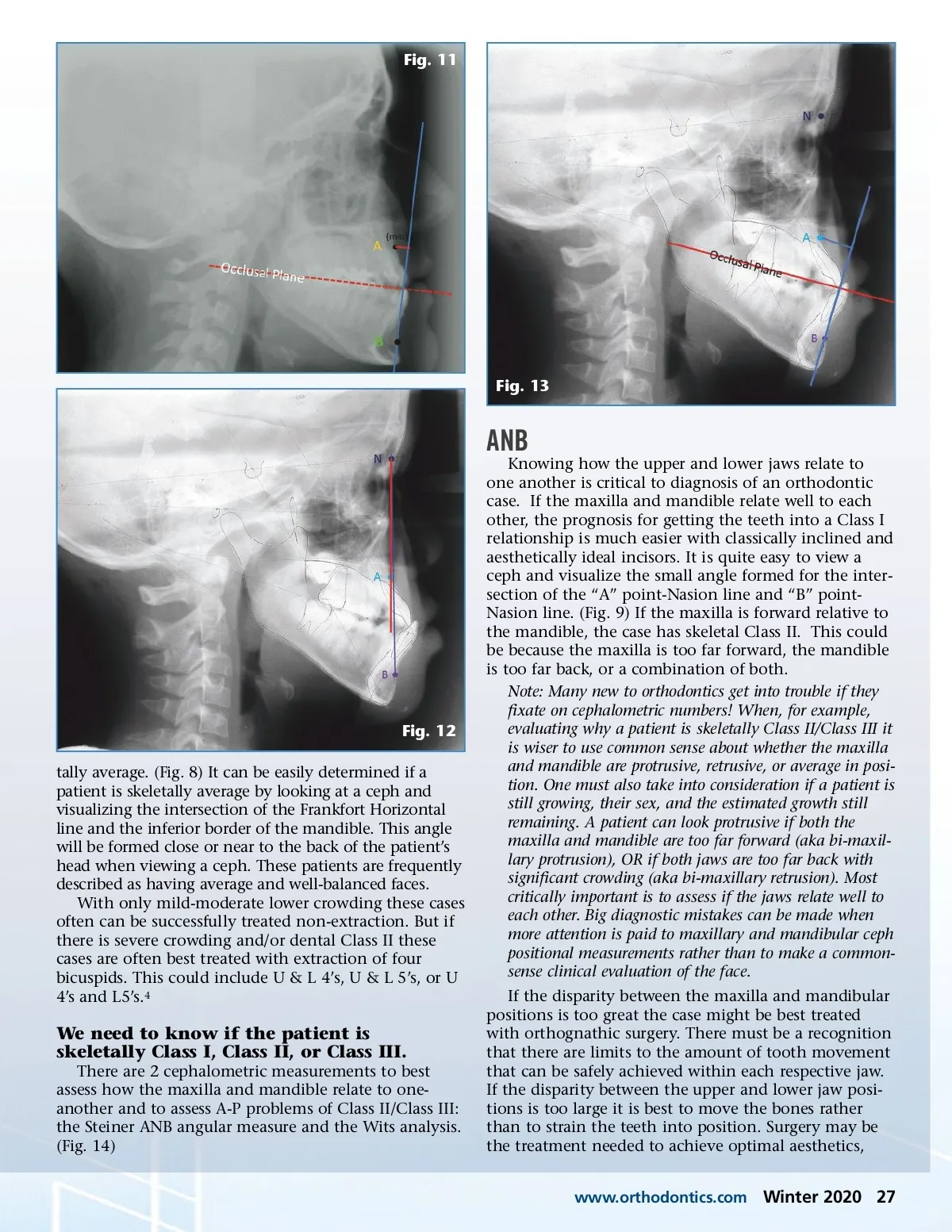
Fig. 11 Fig. 13 ANB Knowing how the upper and lower jaws relate to one another is critical to diagnosis of an orthodontic case. If the maxilla and mandible relate well to each other, the prognosis for getting the teeth into a Class I relationship is much easier with classically inclined and aesthetically ideal incisors. It is quite easy to view a ceph and visualize the small angle formed for the inter-section of the “A” point-Nasion line and “B” point-Nasion line. (Fig. 9) If the maxilla is forward relative to the mandible, the case has skeletal Class II. This could be because the maxilla is too far forward, the mandible is too far back, or a combination of both. Note: Many new to orthodontics get into trouble if they fixate on cephalometric numbers! When, for example, evaluating why a patient is skeletally Class II/Class III it is wiser to use common sense about whether the maxilla and mandible are protrusive, retrusive, or average in posi-tion. One must also take into consideration if a patient is still growing, their sex, and the estimated growth still remaining. A patient can look protrusive if both the maxilla and mandible are too far forward (aka bi-maxil-lary protrusion), OR if both jaws are too far back with significant crowding (aka bi-maxillary retrusion). Most critically important is to assess if the jaws relate well to each other. Big diagnostic mistakes can be made when more attention is paid to maxillary and mandibular ceph positional measurements rather than to make a common-sense clinical evaluation of the face. If the disparity between the maxilla and mandibular positions is too great the case might be best treated with orthognathic surgery. There must be a recognition that there are limits to the amount of tooth movement that can be safely achieved within each respective jaw. If the disparity between the upper and lower jaw posi-tions is too large it is best to move the bones rather than to strain the teeth into position. Surgery may be the treatment needed to achieve optimal aesthetics, www.orthodontics.com Fig. 12 tally average. (Fig. 8) It can be easily determined if a patient is skeletally average by looking at a ceph and visualizing the intersection of the Frankfort Horizontal line and the inferior border of the mandible. This angle will be formed close or near to the back of the patient’s head when viewing a ceph. These patients are frequently described as having average and well-balanced faces. With only mild-moderate lower crowding these cases often can be successfully treated non-extraction. But if there is severe crowding and/or dental Class II these cases are often best treated with extraction of four bicuspids. This could include U & L 4’s, U & L 5’s, or U 4’s and L5’s. 4 We need to know if the patient is skeletally Class I, Class II, or Class III. There are 2 cephalometric measurements to best assess how the maxilla and mandible relate to one-another and to assess A-P problems of Class II/Class III: the Steiner ANB angular measure and the Wits analysis. (Fig. 14) Winter 2020 27
Journal of the American Orthodontic Society Winter 2020: Page 27