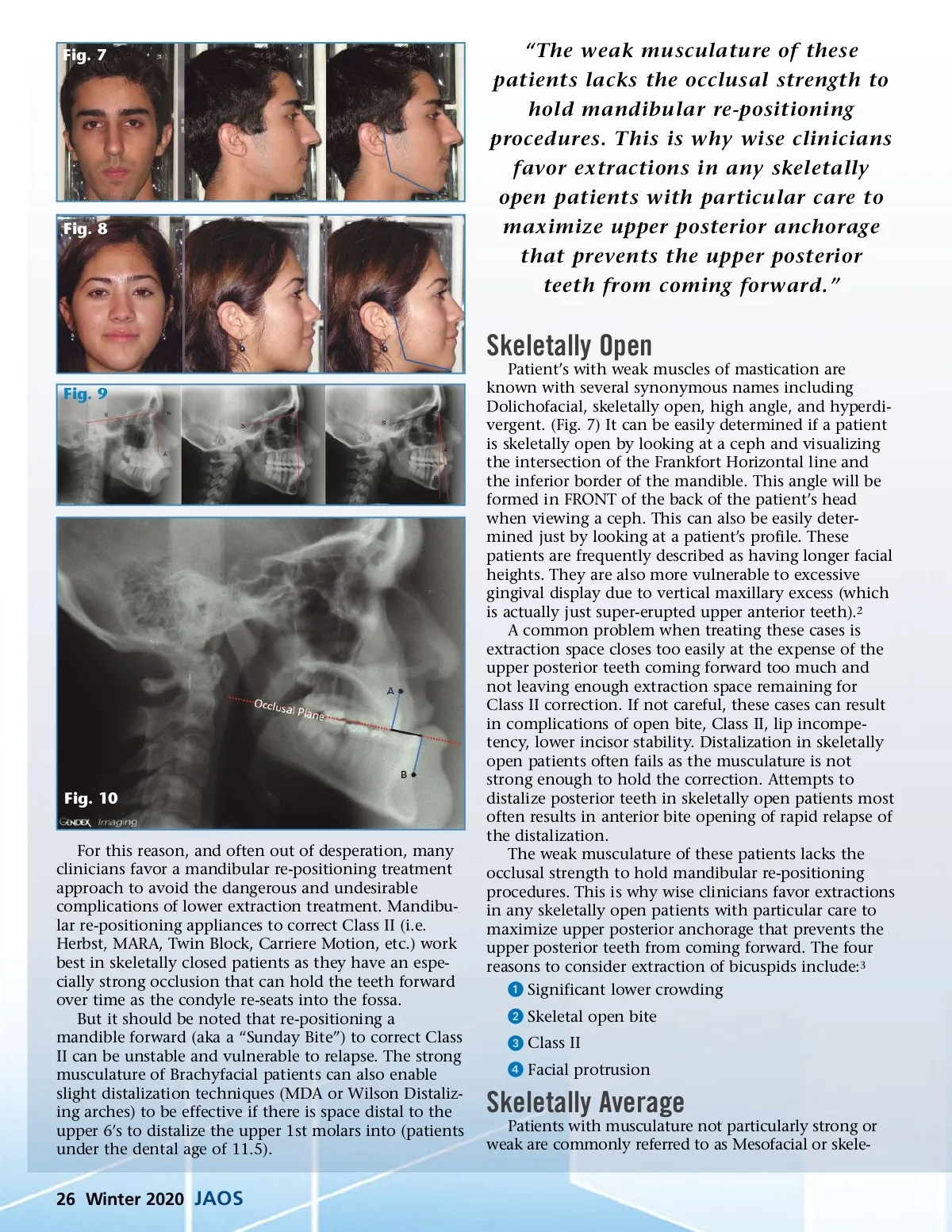
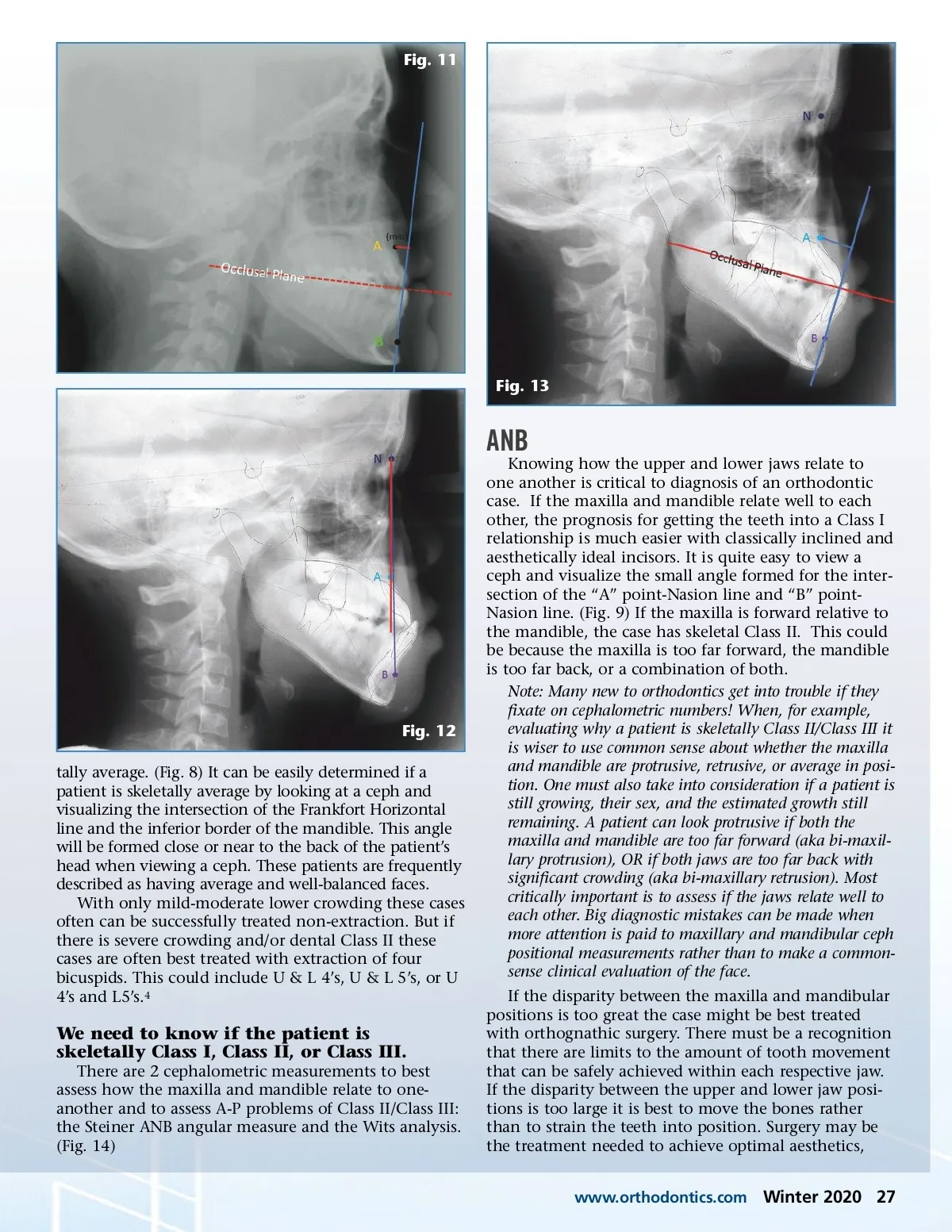
Fig. 7 Fig. 8 “The weak musculature of these patients lacks the occlusal strength to hold mandibular re-positioning procedures. This is why wise clinicians favor extractions in any skeletally open patients with particular care to maximize upper posterior anchorage that prevents the upper posterior teeth from coming forward.” Skeletally Open Fig. 9 Patient’s with weak muscles of mastication are known with several synonymous names including Dolichofacial, skeletally open, high angle, and hyperdi-vergent. (Fig. 7) It can be easily determined if a patient is skeletally open by looking at a ceph and visualizing the intersection of the Frankfort Horizontal line and the inferior border of the mandible. This angle will be formed in FRONT of the back of the patient’s head when viewing a ceph. This can also be easily deter-mined just by looking at a patient’s profile. These patients are frequently described as having longer facial heights. They are also more vulnerable to excessive gingival display due to vertical maxillary excess (which is actually just super-erupted upper anterior teeth). 2 A common problem when treating these cases is extraction space closes too easily at the expense of the upper posterior teeth coming forward too much and not leaving enough extraction space remaining for Class II correction. If not careful, these cases can result in complications of open bite, Class II, lip incompe-tency, lower incisor stability. Distalization in skeletally open patients often fails as the musculature is not strong enough to hold the correction. Attempts to distalize posterior teeth in skeletally open patients most often results in anterior bite opening of rapid relapse of the distalization. The weak musculature of these patients lacks the occlusal strength to hold mandibular re-positioning procedures. This is why wise clinicians favor extractions in any skeletally open patients with particular care to maximize upper posterior anchorage that prevents the upper posterior teeth from coming forward. The four reasons to consider extraction of bicuspids include: 3 ᕡ Significant lower crowding ᕢ Skeletal open bite ᕣ Class II ᕤ Facial protrusion Fig. 10 For this reason, and often out of desperation, many clinicians favor a mandibular re-positioning treatment approach to avoid the dangerous and undesirable complications of lower extraction treatment. Mandibu-lar re-positioning appliances to correct Class II (i.e. Herbst, MARA, Twin Block, Carriere Motion, etc.) work best in skeletally closed patients as they have an espe-cially strong occlusion that can hold the teeth forward over time as the condyle re-seats into the fossa. But it should be noted that re-positioning a mandible forward (aka a “Sunday Bite”) to correct Class II can be unstable and vulnerable to relapse. The strong musculature of Brachyfacial patients can also enable slight distalization techniques (MDA or Wilson Distaliz-ing arches) to be effective if there is space distal to the upper 6’s to distalize the upper 1st molars into (patients under the dental age of 11.5). Skeletally Average Patients with musculature not particularly strong or weak are commonly referred to as Mesofacial or skele-26 Winter 2020 JAOS
Journal of the American Orthodontic Society Winter 2020: Page 26