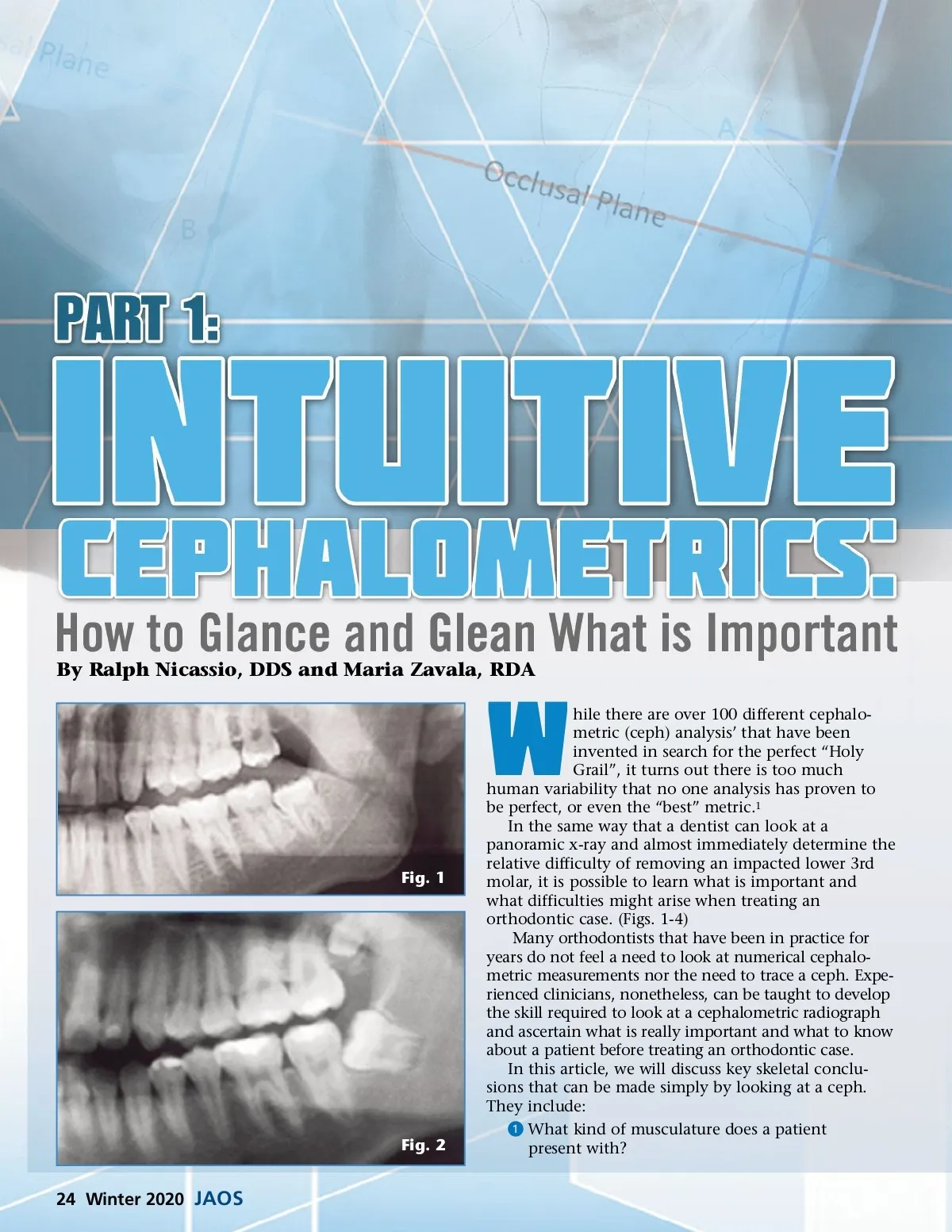
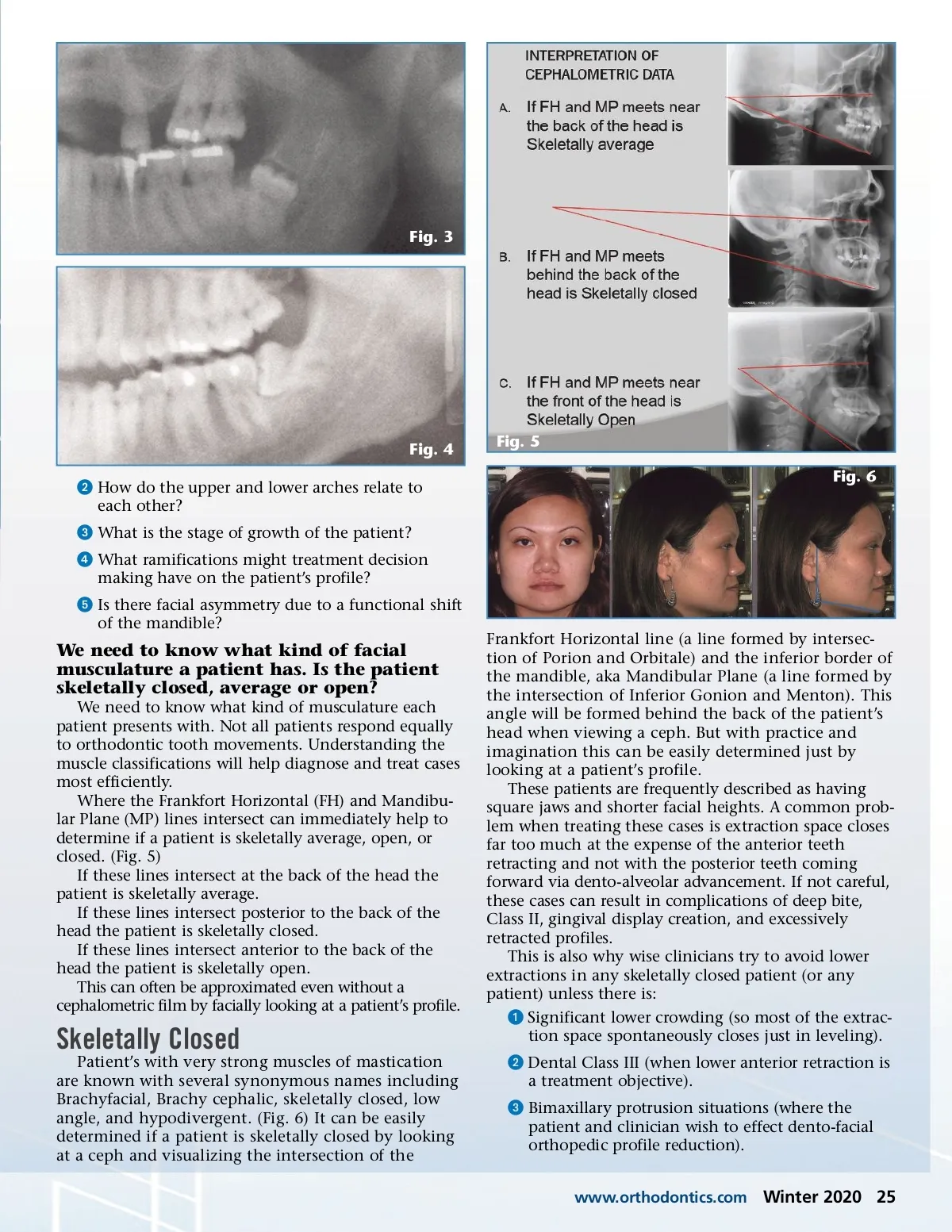
Fig. 3 Fig. 4 ᕢ How do the upper and lower arches relate to each other? ᕣ What is the stage of growth of the patient? ᕤ What ramifications might treatment decision making have on the patient’s profile? ᕥ Is there facial asymmetry due to a functional shift of the mandible? Fig. 5 Fig. 6 We need to know what kind of facial musculature a patient has. Is the patient skeletally closed, average or open? We need to know what kind of musculature each patient presents with. Not all patients respond equally to orthodontic tooth movements. Understanding the muscle classifications will help diagnose and treat cases most efficiently. Where the Frankfort Horizontal (FH) and Mandibu-lar Plane (MP) lines intersect can immediately help to determine if a patient is skeletally average, open, or closed. (Fig. 5) If these lines intersect at the back of the head the patient is skeletally average. If these lines intersect posterior to the back of the head the patient is skeletally closed. If these lines intersect anterior to the back of the head the patient is skeletally open. This can often be approximated even without a cephalometric film by facially looking at a patient’s profile. Skeletally Closed Patient’s with very strong muscles of mastication are known with several synonymous names including Brachyfacial, Brachy cephalic, skeletally closed, low angle, and hypodivergent. (Fig. 6) It can be easily determined if a patient is skeletally closed by looking at a ceph and visualizing the intersection of the Frankfort Horizontal line (a line formed by intersec-tion of Porion and Orbitale) and the inferior border of the mandible, aka Mandibular Plane (a line formed by the intersection of Inferior Gonion and Menton). This angle will be formed behind the back of the patient’s head when viewing a ceph. But with practice and imagination this can be easily determined just by looking at a patient’s profile. These patients are frequently described as having square jaws and shorter facial heights. A common prob-lem when treating these cases is extraction space closes far too much at the expense of the anterior teeth retracting and not with the posterior teeth coming forward via dento-alveolar advancement. If not careful, these cases can result in complications of deep bite, Class II, gingival display creation, and excessively retracted profiles. This is also why wise clinicians try to avoid lower extractions in any skeletally closed patient (or any patient) unless there is: ᕡ Significant lower crowding (so most of the extrac-tion space spontaneously closes just in leveling). ᕢ Dental Class III (when lower anterior retraction is a treatment objective). ᕣ Bimaxillary protrusion situations (where the patient and clinician wish to effect dento-facial orthopedic profile reduction). www.orthodontics.com Winter 2020 25
Journal of the American Orthodontic Society Winter 2020: Page 25