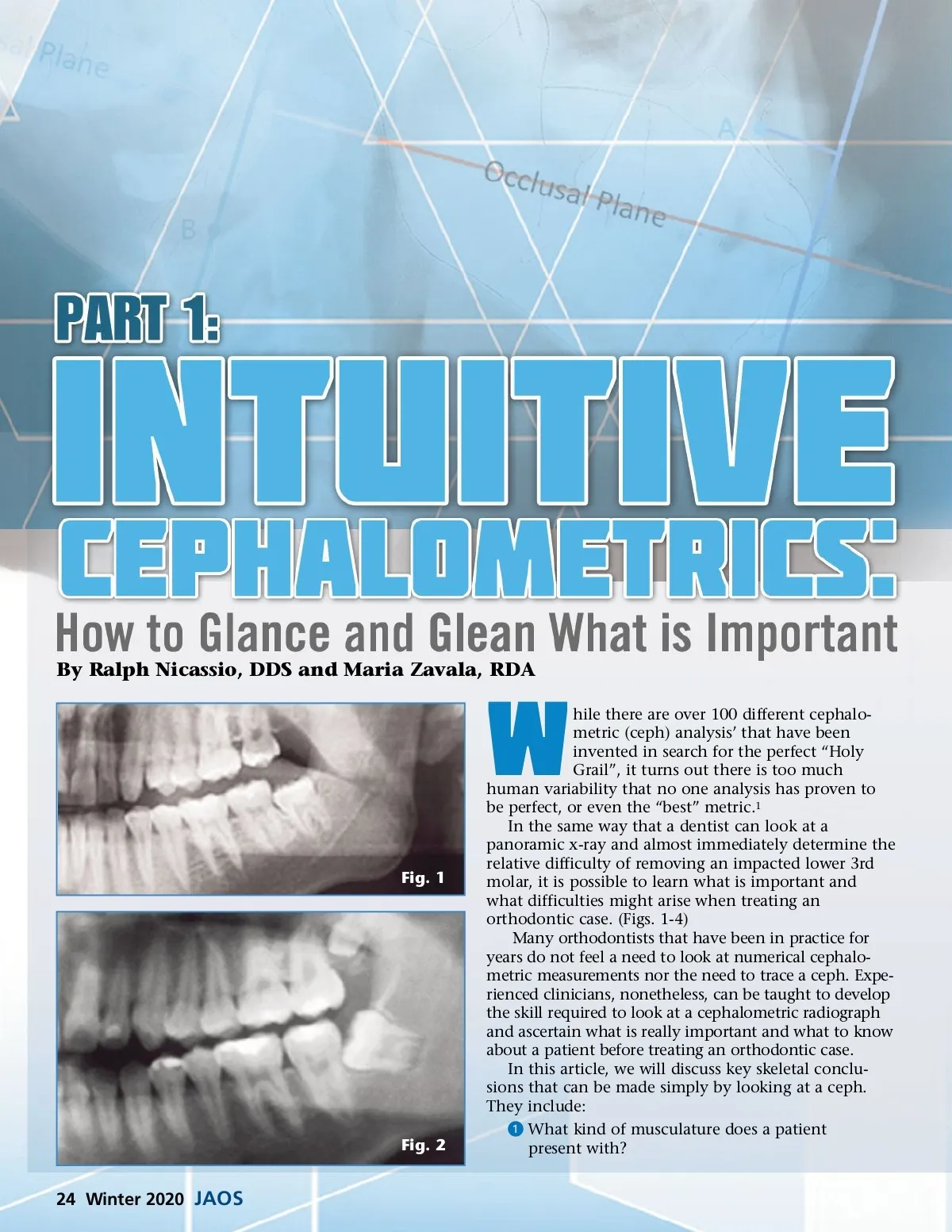
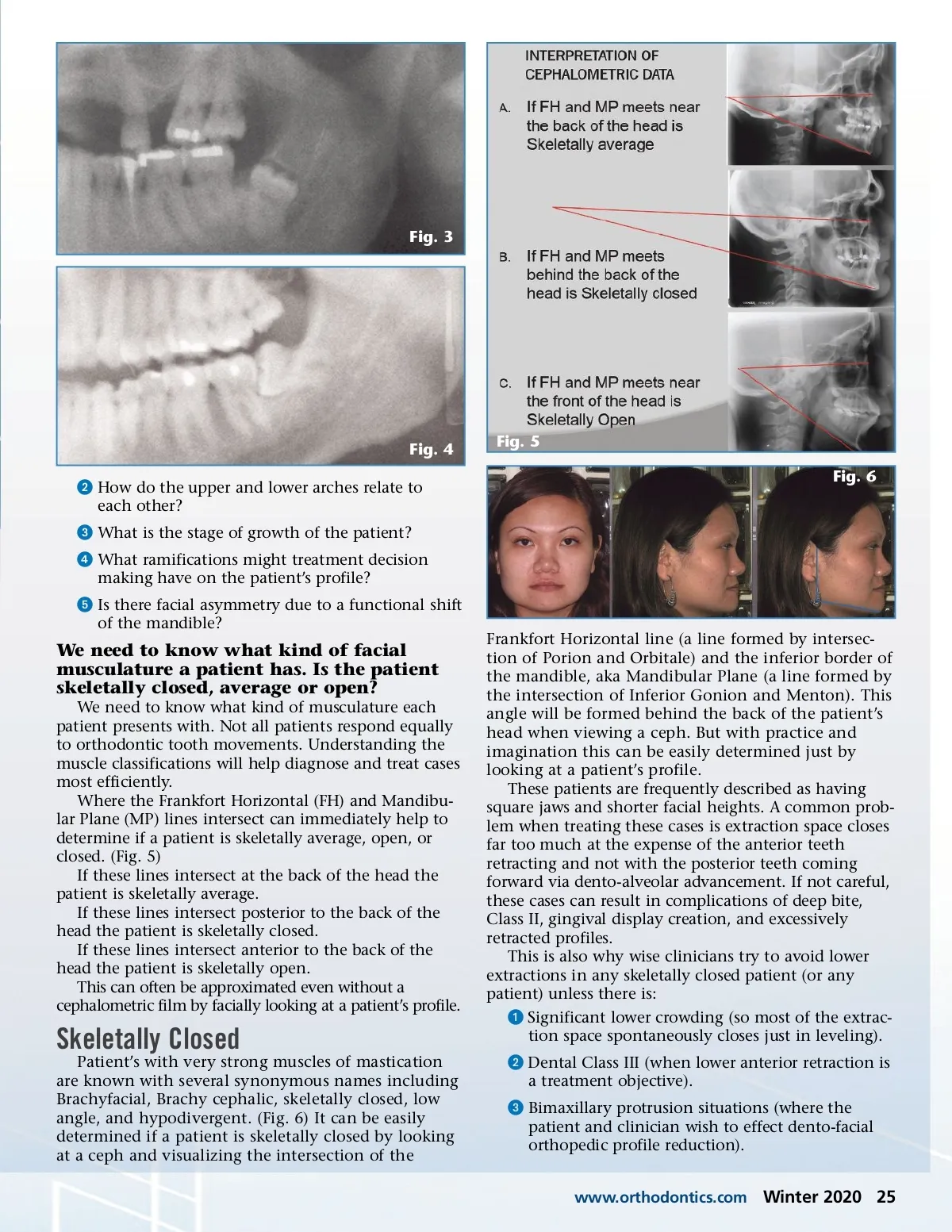
By Ralph Nicassio, DDS and Maria Zavala, RDA hile there are over 100 different cephalo-metric (ceph) analysis’ that have been invented in search for the perfect “Holy Grail”, it turns out there is too much human variability that no one analysis has proven to be perfect, or even the “best” metric. 1 In the same way that a dentist can look at a panoramic x-ray and almost immediately determine the relative difficulty of removing an impacted lower 3rd molar, it is possible to learn what is important and what difficulties might arise when treating an orthodontic case. (Figs. 1-4) Many orthodontists that have been in practice for years do not feel a need to look at numerical cephalo-metric measurements nor the need to trace a ceph. Expe-rienced clinicians, nonetheless, can be taught to develop the skill required to look at a cephalometric radiograph and ascertain what is really important and what to know about a patient before treating an orthodontic case. In this article, we will discuss key skeletal conclu-sions that can be made simply by looking at a ceph. They include: ᕡ What kind of musculature does a patient present with? W Fig. 1 Fig. 2 24 Winter 2020 JAOS
Journal of the American Orthodontic Society Winter 2020: Page 24