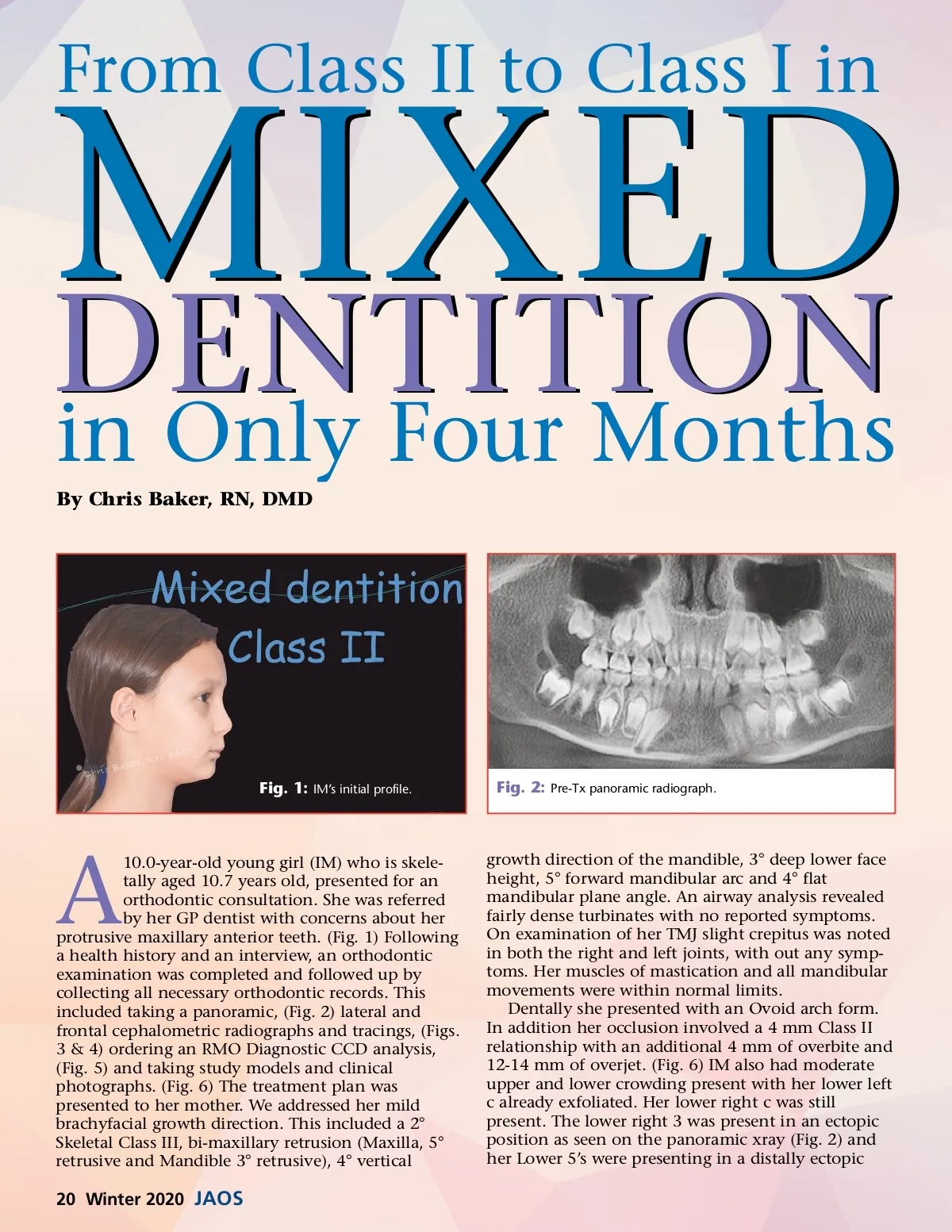
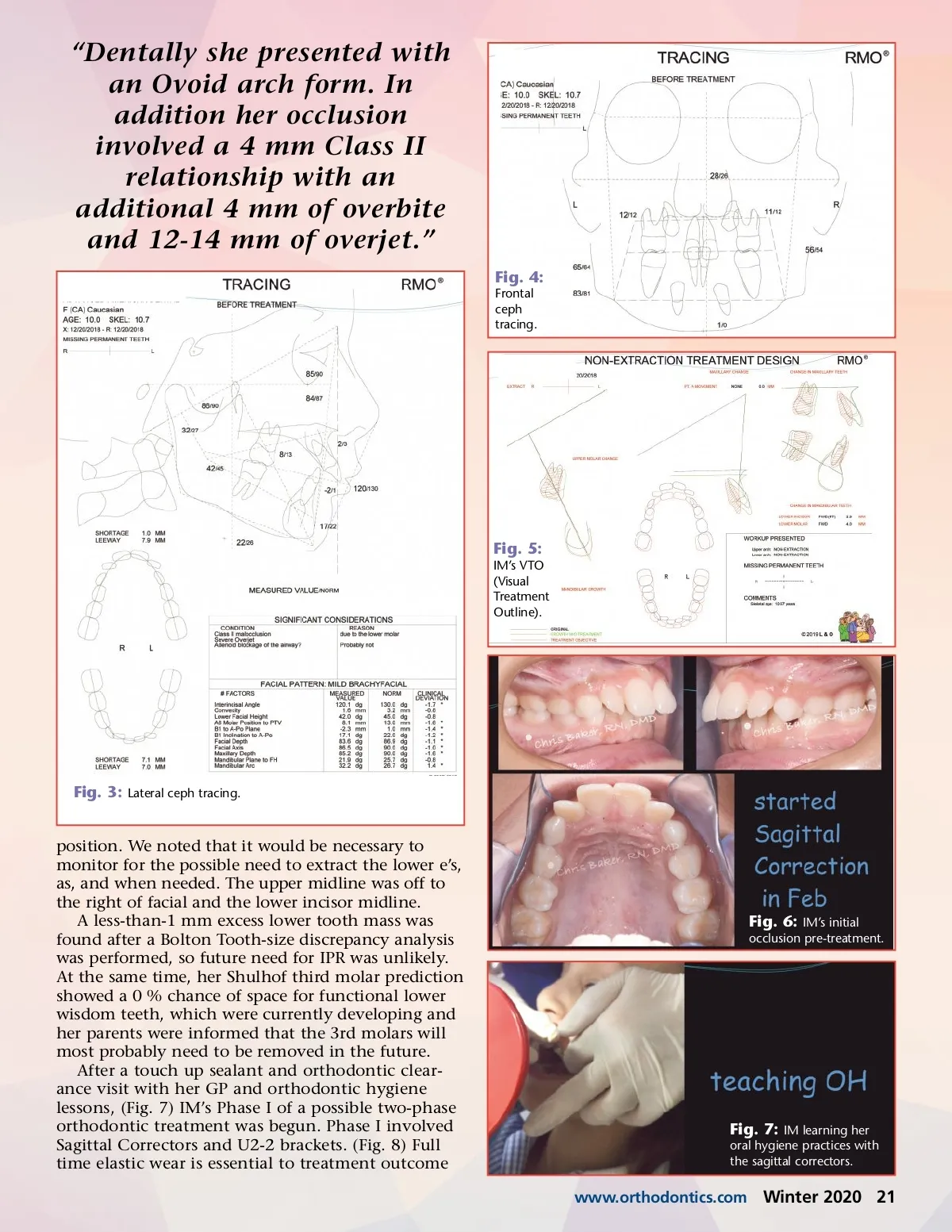
“Dentally she presented with an Ovoid arch form. In addition her occlusion involved a 4 mm Class II relationship with an additional 4 mm of overbite and 12-14 mm of overjet.” Fig. 4: Frontal ceph tracing. Fig. 5: IM’s VTO (Visual Treatment Outline). Fig. 3: Lateral ceph tracing. position. We noted that it would be necessary to monitor for the possible need to extract the lower e’s, as, and when needed. The upper midline was off to the right of facial and the lower incisor midline. A less-than-1 mm excess lower tooth mass was found after a Bolton Tooth-size discrepancy analysis was performed, so future need for IPR was unlikely. At the same time, her Shulhof third molar prediction showed a 0 % chance of space for functional lower wisdom teeth, which were currently developing and her parents were informed that the 3rd molars will most probably need to be removed in the future. After a touch up sealant and orthodontic clear-ance visit with her GP and orthodontic hygiene lessons, (Fig. 7) IM’s Phase I of a possible two-phase orthodontic treatment was begun. Phase I involved Sagittal Correctors and U2-2 brackets. (Fig. 8) Full time elastic wear is essential to treatment outcome Fig. 6: IM’s initial occlusion pre-treatment. Fig. 7: IM learning her oral hygiene practices with the sagittal correctors. www.orthodontics.com Winter 2020 21
Journal of the American Orthodontic Society Winter 2020: Page 21