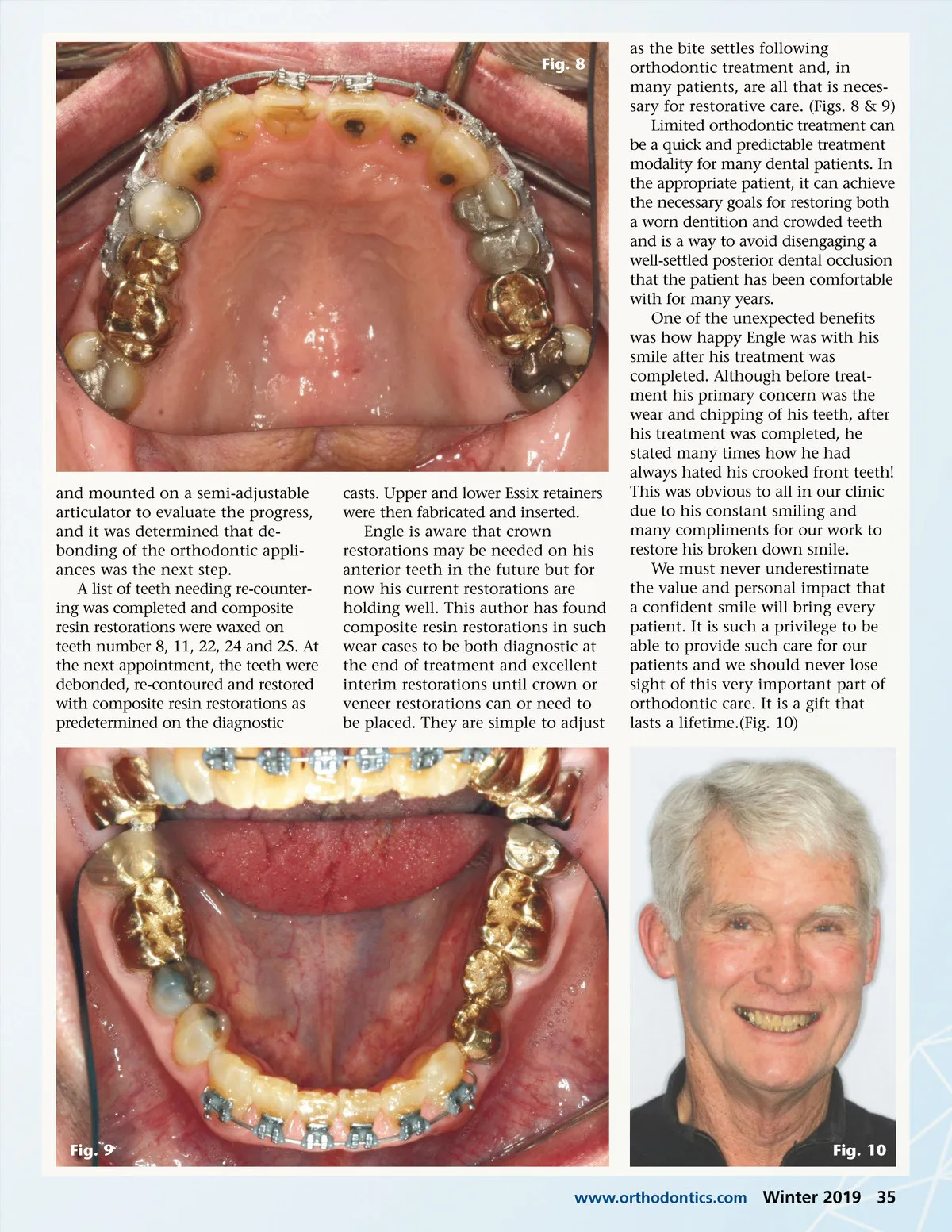
Fig. 5 of MBT brackets (with .022 slot size), which have slightly increased torque of the upper incisors and decrease torque of the lower incisors would facilitate establishing a normal over-jet relationship. Upper arch would be bonded 5 to 5 and lower arch bonded 3 to 3 with interproximal reduction and keystoning the inter-proximal contacts for greater stabil-ity postoperatively. The third option was for full upper and lower straight wire appliances and opening of the vertical dimen-sion of occlusion with the appliances. The upper and lower central incisors would be built up with composite also formed into the shape of an incisal block on the lingual of number 8 and 9. The lower posterior teeth would then be erupted to the new vertical position and a straight wire series completed. Sectioning of the lower left bridge may be necessary to allow eruption of these teeth. The final treatment option was to open the vertical dimension of occlusion prosthetically with fixed restorations throughout the upper and lower arches.(Figs. 6 &7) PATIENT TREATMENT Fig. 6 Engle chose the second option and treatment was completed in 10 months. Treatment progres-sion follows: At this first appointment, bond-ing of the prescribed teeth took place and an upper .014N and a lower .014TN wire were placed. One month later, the incisors were ligated firmly to allow greater rota-tion and continued correction of crowding. Eight weeks later, arch wires were changed to an upper .018N and a lower .018TN. Eight weeks after that, a 19x25TN (lower archwire) was placed in the upper arch and the lower was left unchanged. One month later, the lower incisors were slimmed interproxi-mally, and a .018S wire was placed with power chain 3-3. Four weeks later, the lower incisors were again slimmed, and a light inter-arch elas-tic was prescribed to close the open bite in the left canine area. Approxi-mately one month later, upper and lower diagnostic casts were made Fig. 7 TREATMENT OPTIONS After examination of Engle and evaluation of Engle’s orthodontic records the following treatment options were presented: The first option presented was Invisalign for both the upper and lower arches with the goals of the rotating the upper anterior teeth and proclaiming them slightly with slight intrusion if possible. Intru-sion of the lower incisors of approx-imately 1 mm with interproximal reduction as needed. The rotation of the upper central incisors will be somewhat difficult with Invisalign. The second option was for limited upper and lower fixed straight wire appliances holding the current vertical dimension. The use 34 Winter 2019 JAOS
Journal of the American Orthodontic Society Winter 2019: Page 34