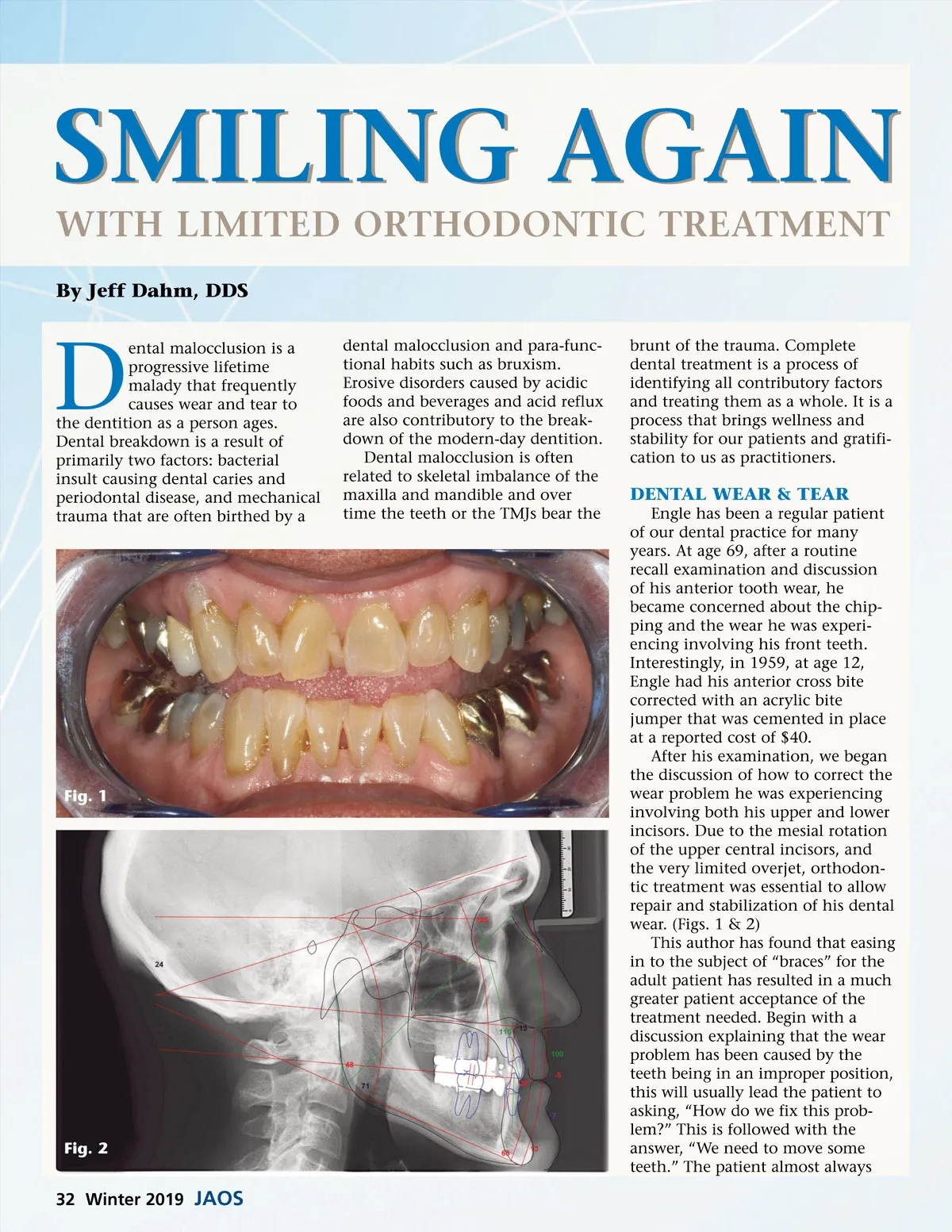
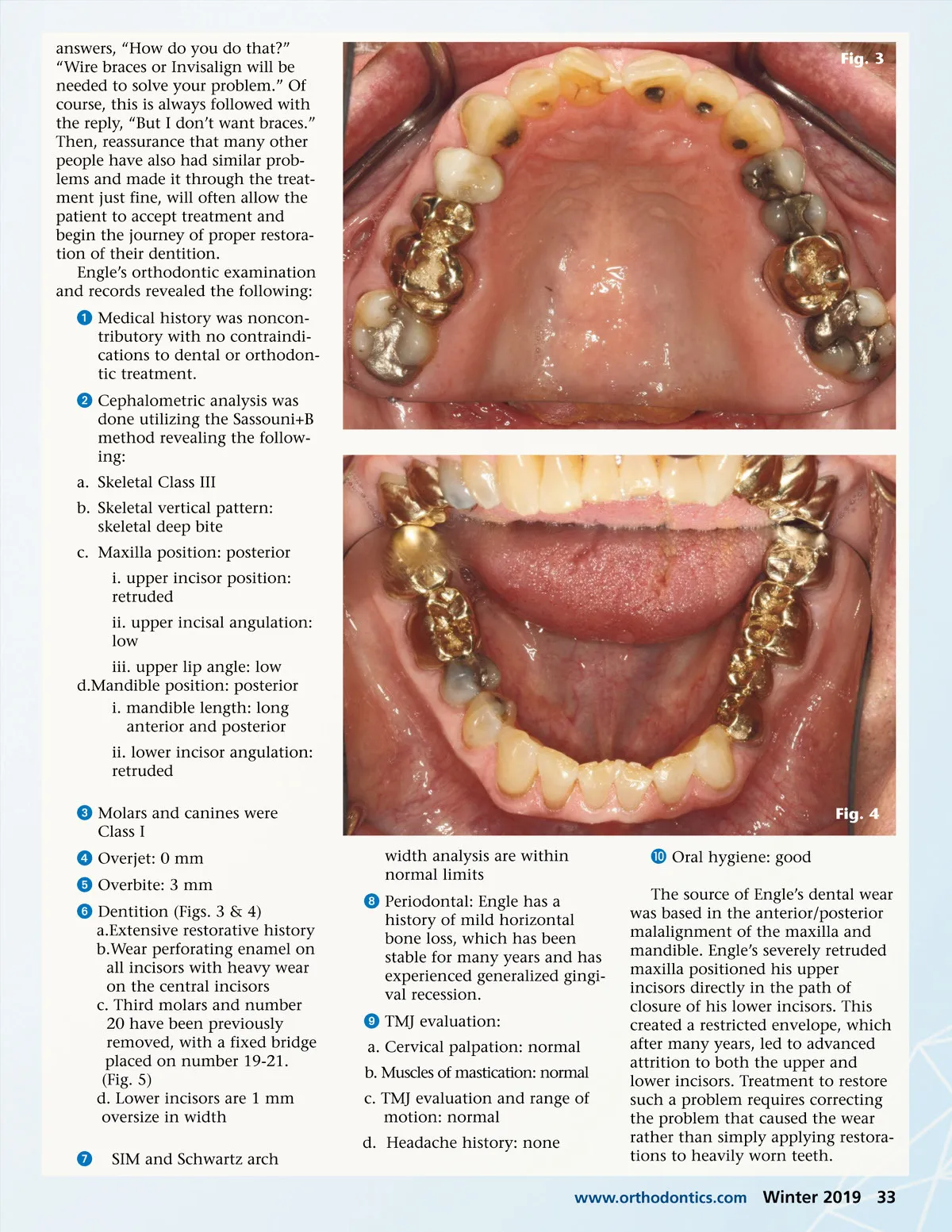
answers, “How do you do that?” “Wire braces or Invisalign will be needed to solve your problem.” Of course, this is always followed with the reply, “But I don’t want braces.” Then, reassurance that many other people have also had similar prob-lems and made it through the treat-ment just fine, will often allow the patient to accept treatment and begin the journey of proper restora-tion of their dentition. Engle’s orthodontic examination and records revealed the following: ᕡ Medical history was noncon-tributory with no contraindi-cations to dental or orthodon-tic treatment. ᕢ Cephalometric analysis was done utilizing the Sassouni+B method revealing the follow-ing: a. Skeletal Class III b. Skeletal vertical pattern: skeletal deep bite c. Maxilla position: posterior i. upper incisor position: retruded ii. upper incisal angulation: low iii. upper lip angle: low d.Mandible position: posterior i. mandible length: long anterior and posterior ii. lower incisor angulation: retruded ᕣ Molars and canines were Class I ᕤ Overjet: 0 mm ᕥ Overbite: 3 mm ᕦ Dentition (Figs. 3 & 4) a.Extensive restorative history b.Wear perforating enamel on all incisors with heavy wear on the central incisors c. Third molars and number 20 have been previously removed, with a fixed bridge placed on number 19-21. (Fig. 5) d. Lower incisors are 1 mm oversize in width ᕧ SIM and Schwartz arch width analysis are within normal limits ᕨ Periodontal: Engle has a history of mild horizontal bone loss, which has been stable for many years and has experienced generalized gingi-val recession. ᕩ TMJ evaluation: a. Cervical palpation: normal b. Muscles of mastication: normal c. TMJ evaluation and range of motion: normal d. Headache history: none µ Oral hygiene: good Fig. 3 Fig. 4 The source of Engle’s dental wear was based in the anterior/posterior malalignment of the maxilla and mandible. Engle’s severely retruded maxilla positioned his upper incisors directly in the path of closure of his lower incisors. This created a restricted envelope, which after many years, led to advanced attrition to both the upper and lower incisors. Treatment to restore such a problem requires correcting the problem that caused the wear rather than simply applying restora-tions to heavily worn teeth. www.orthodontics.com Winter 2019 33
Journal of the American Orthodontic Society Winter 2019: Page 33