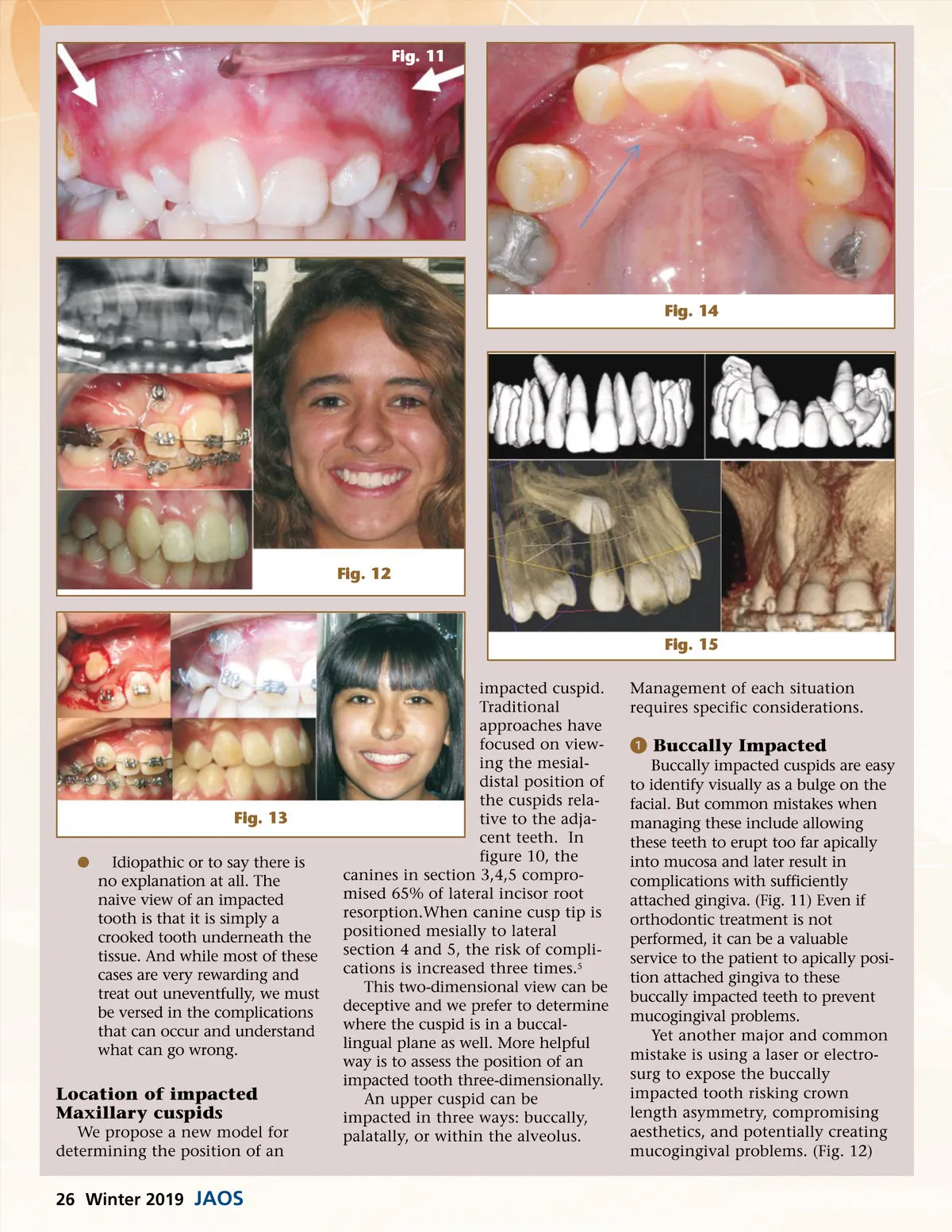
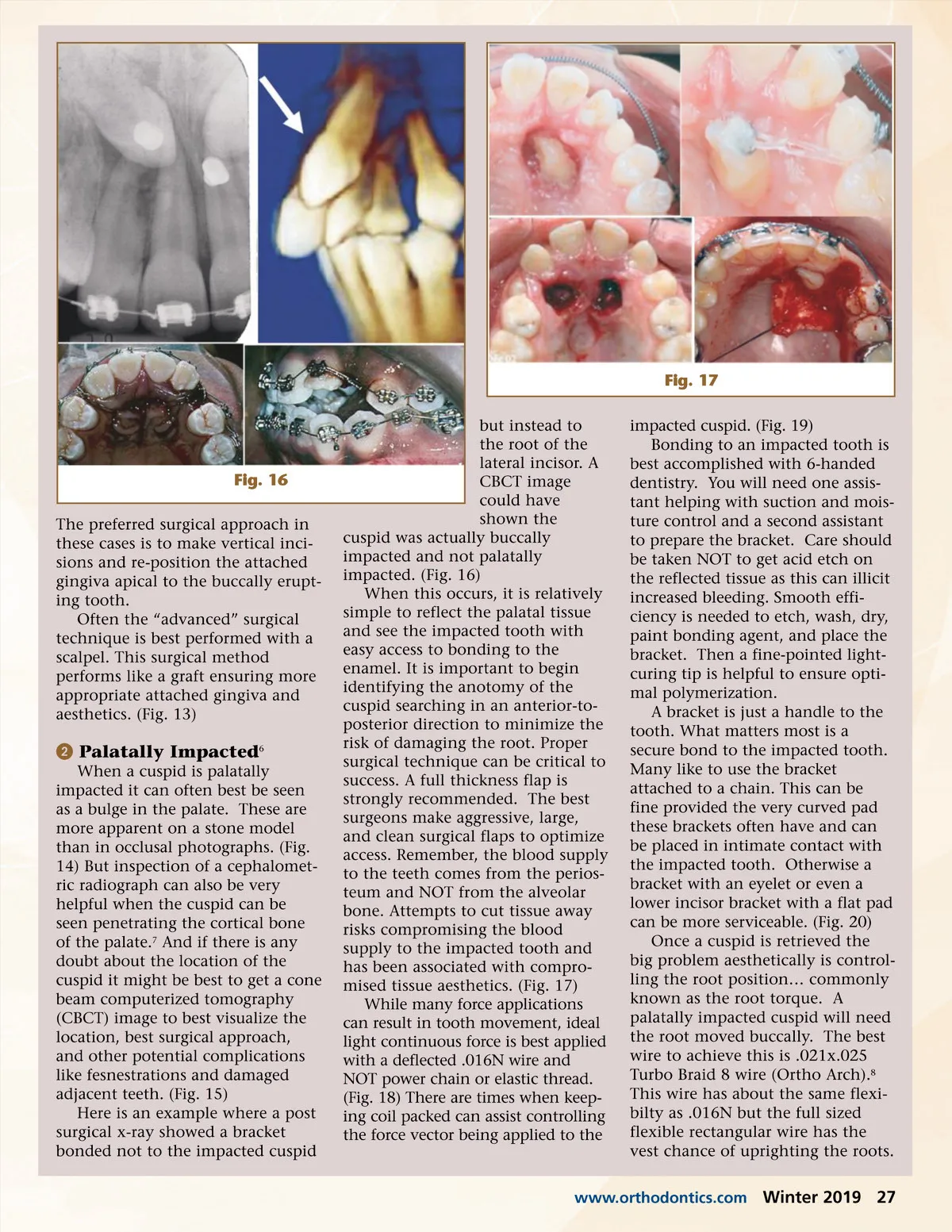
Fig. 11 Fig. 14 Fig. 12 Fig. 15 impacted cuspid. Traditional approaches have focused on view-ing the mesial-distal position of the cuspids rela-tive to the adja-cent teeth. In figure 10, the canines in section 3,4,5 compro-mised 65% of lateral incisor root resorption.When canine cusp tip is positioned mesially to lateral section 4 and 5, the risk of compli-cations is increased three times. 5 This two-dimensional view can be deceptive and we prefer to determine where the cuspid is in a buccal-lingual plane as well. More helpful way is to assess the position of an impacted tooth three-dimensionally. An upper cuspid can be impacted in three ways: buccally, palatally, or within the alveolus. Management of each situation requires specific considerations. ᕡ Buccally Impacted Buccally impacted cuspids are easy to identify visually as a bulge on the facial. But common mistakes when managing these include allowing these teeth to erupt too far apically into mucosa and later result in complications with sufficiently attached gingiva. (Fig. 11) Even if orthodontic treatment is not performed, it can be a valuable service to the patient to apically posi-tion attached gingiva to these buccally impacted teeth to prevent mucogingival problems. Yet another major and common mistake is using a laser or electro-surg to expose the buccally impacted tooth risking crown length asymmetry, compromising aesthetics, and potentially creating mucogingival problems. (Fig. 12) Fig. 13 b Idiopathic or to say there is no explanation at all. The naive view of an impacted tooth is that it is simply a crooked tooth underneath the tissue. And while most of these cases are very rewarding and treat out uneventfully, we must be versed in the complications that can occur and understand what can go wrong. Location of impacted Maxillary cuspids We propose a new model for determining the position of an 26 Winter 2019 JAOS
Journal of the American Orthodontic Society Winter 2019: Page 26