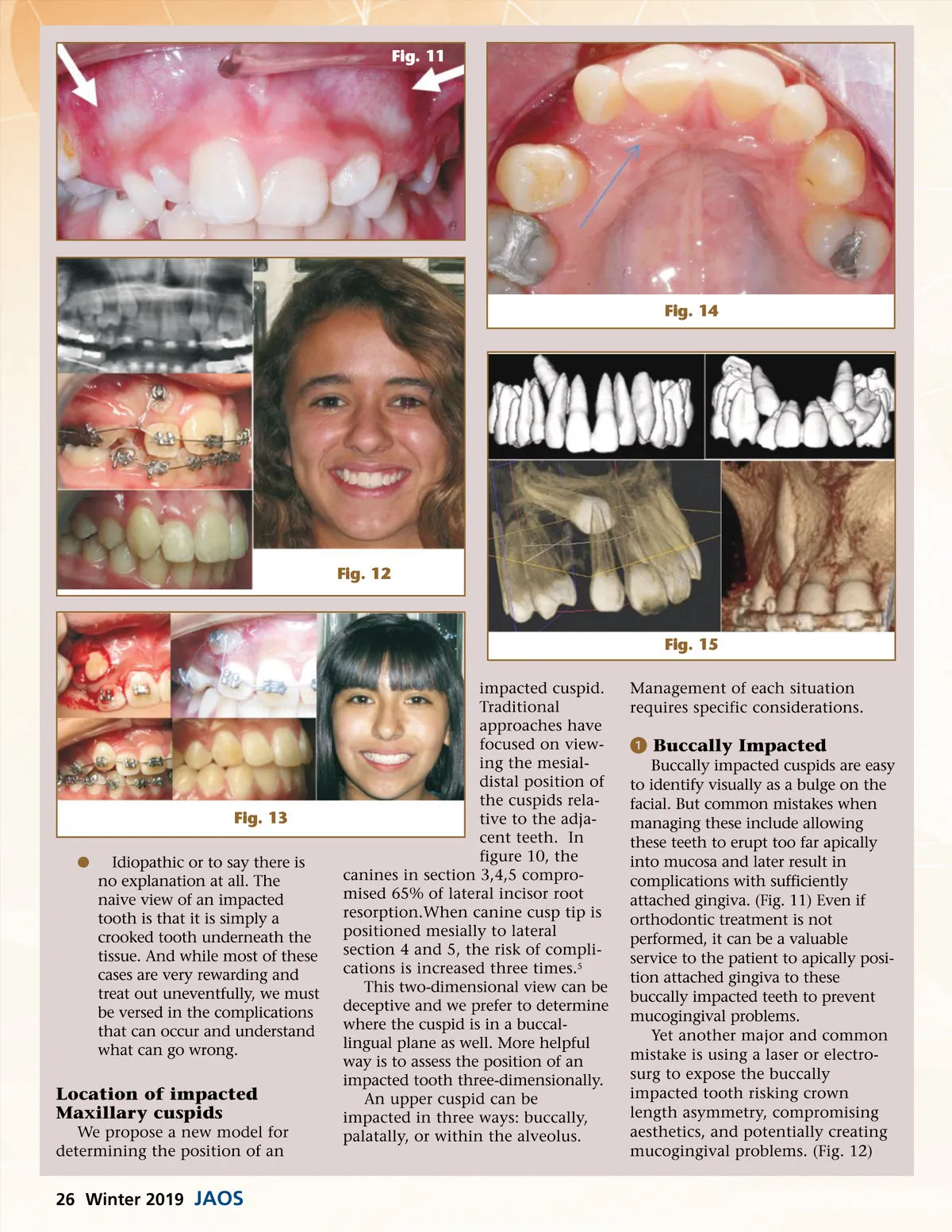
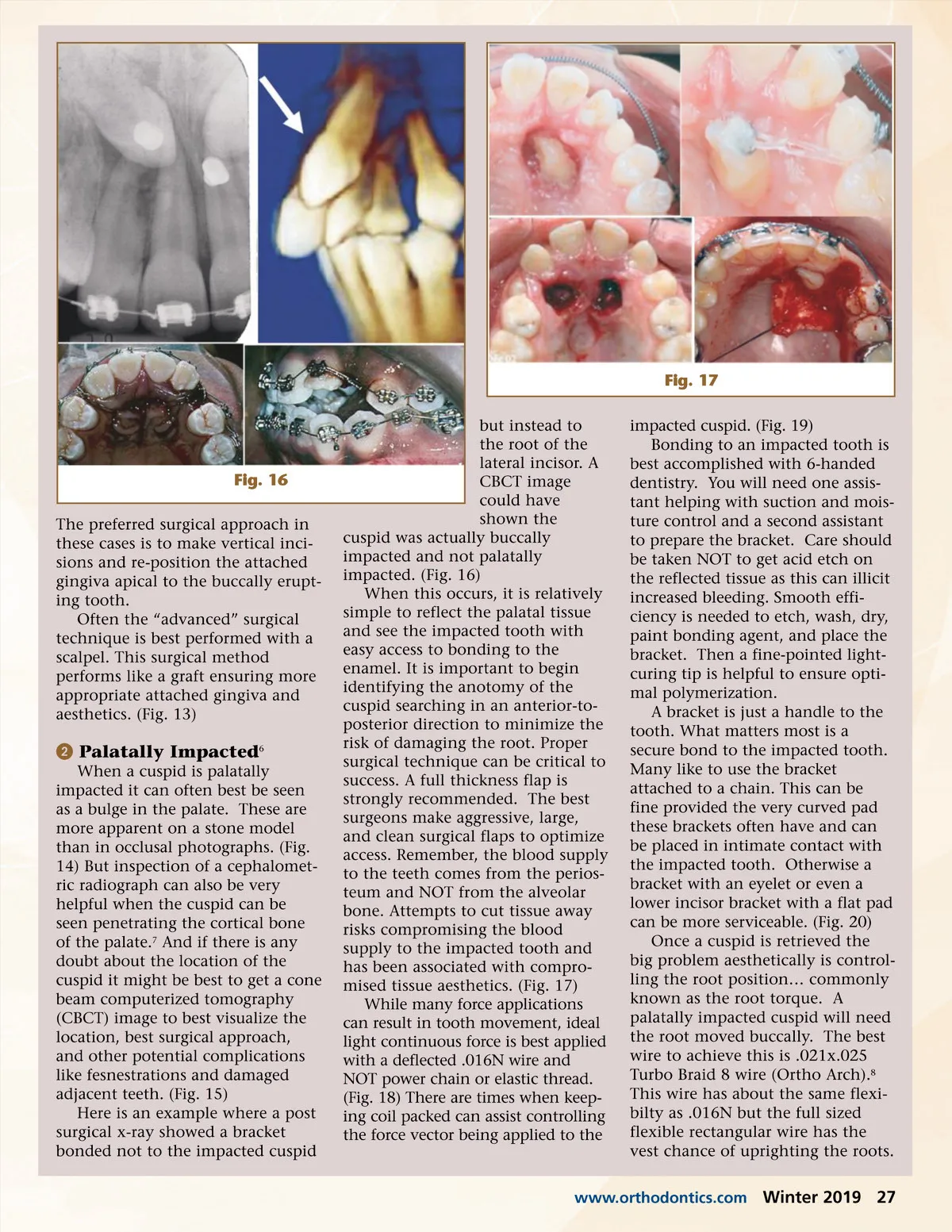
Fig. 17 but instead to the root of the lateral incisor. A CBCT image could have shown the cuspid was actually buccally impacted and not palatally impacted. (Fig. 16) When this occurs, it is relatively simple to reflect the palatal tissue and see the impacted tooth with easy access to bonding to the enamel. It is important to begin identifying the anotomy of the cuspid searching in an anterior-to-posterior direction to minimize the risk of damaging the root. Proper surgical technique can be critical to success. A full thickness flap is strongly recommended. The best surgeons make aggressive, large, and clean surgical flaps to optimize access. Remember, the blood supply to the teeth comes from the perios-teum and NOT from the alveolar bone. Attempts to cut tissue away risks compromising the blood supply to the impacted tooth and has been associated with compro-mised tissue aesthetics. (Fig. 17) While many force applications can result in tooth movement, ideal light continuous force is best applied with a deflected .016N wire and NOT power chain or elastic thread. (Fig. 18) There are times when keep-ing coil packed can assist controlling the force vector being applied to the impacted cuspid. (Fig. 19) Bonding to an impacted tooth is best accomplished with 6-handed dentistry. You will need one assis-tant helping with suction and mois-ture control and a second assistant to prepare the bracket. Care should be taken NOT to get acid etch on the reflected tissue as this can illicit increased bleeding. Smooth effi-ciency is needed to etch, wash, dry, paint bonding agent, and place the bracket. Then a fine-pointed light-curing tip is helpful to ensure opti-mal polymerization. A bracket is just a handle to the tooth. What matters most is a secure bond to the impacted tooth. Many like to use the bracket attached to a chain. This can be fine provided the very curved pad these brackets often have and can be placed in intimate contact with the impacted tooth. Otherwise a bracket with an eyelet or even a lower incisor bracket with a flat pad can be more serviceable. (Fig. 20) Once a cuspid is retrieved the big problem aesthetically is control-ling the root position… commonly known as the root torque. A palatally impacted cuspid will need the root moved buccally. The best wire to achieve this is .021x.025 Turbo Braid 8 wire (Ortho Arch). 8 This wire has about the same flexi-bilty as .016N but the full sized flexible rectangular wire has the vest chance of uprighting the roots. Fig. 16 The preferred surgical approach in these cases is to make vertical inci-sions and re-position the attached gingiva apical to the buccally erupt-ing tooth. Often the “advanced” surgical technique is best performed with a scalpel. This surgical method performs like a graft ensuring more appropriate attached gingiva and aesthetics. (Fig. 13) ᕢ Palatally Impacted 6 When a cuspid is palatally impacted it can often best be seen as a bulge in the palate. These are more apparent on a stone model than in occlusal photographs. (Fig. 14) But inspection of a cephalomet-ric radiograph can also be very helpful when the cuspid can be seen penetrating the cortical bone of the palate. 7 And if there is any doubt about the location of the cuspid it might be best to get a cone beam computerized tomography (CBCT) image to best visualize the location, best surgical approach, and other potential complications like fesnestrations and damaged adjacent teeth. (Fig. 15) Here is an example where a post surgical x-ray showed a bracket bonded not to the impacted cuspid www.orthodontics.com Winter 2019 27
Journal of the American Orthodontic Society Winter 2019: Page 27