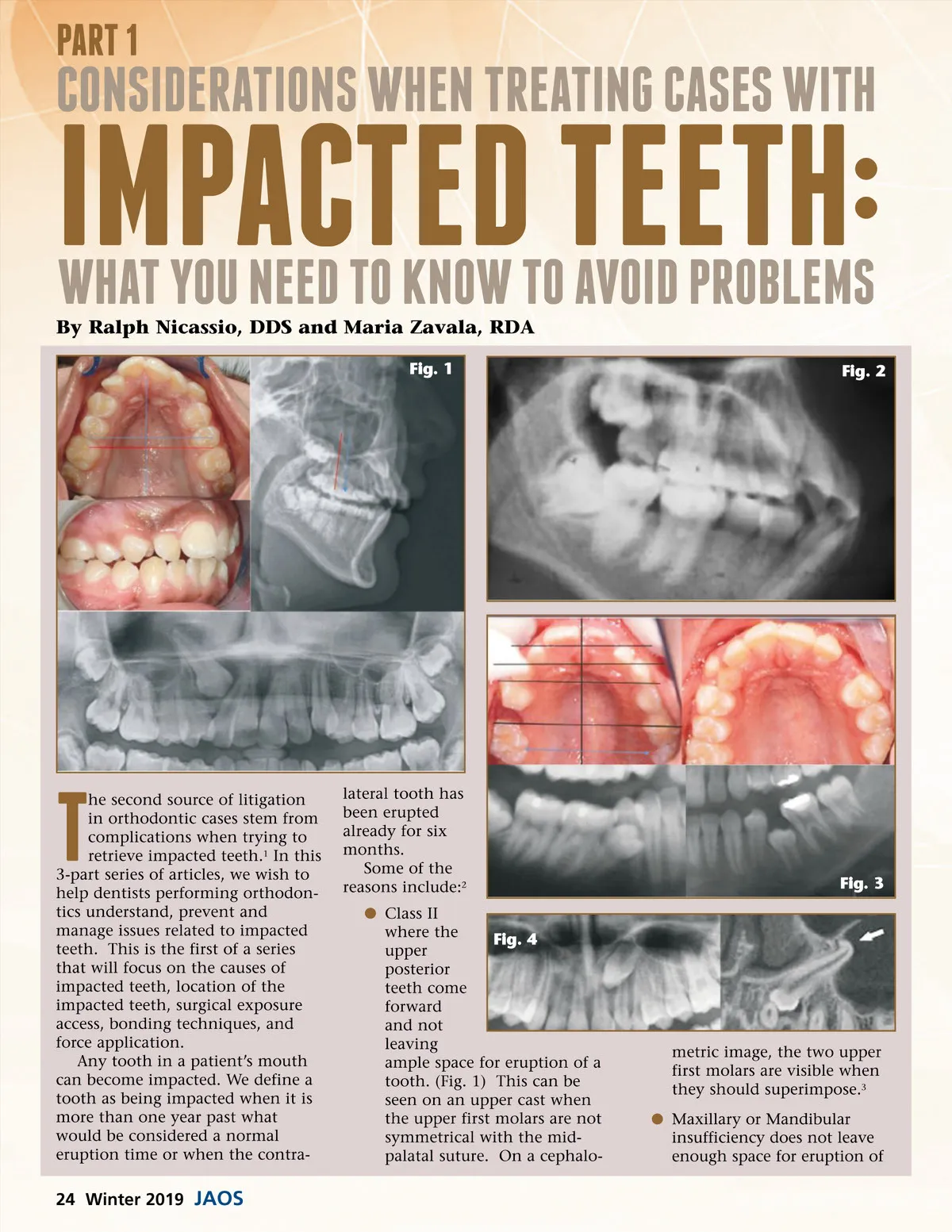
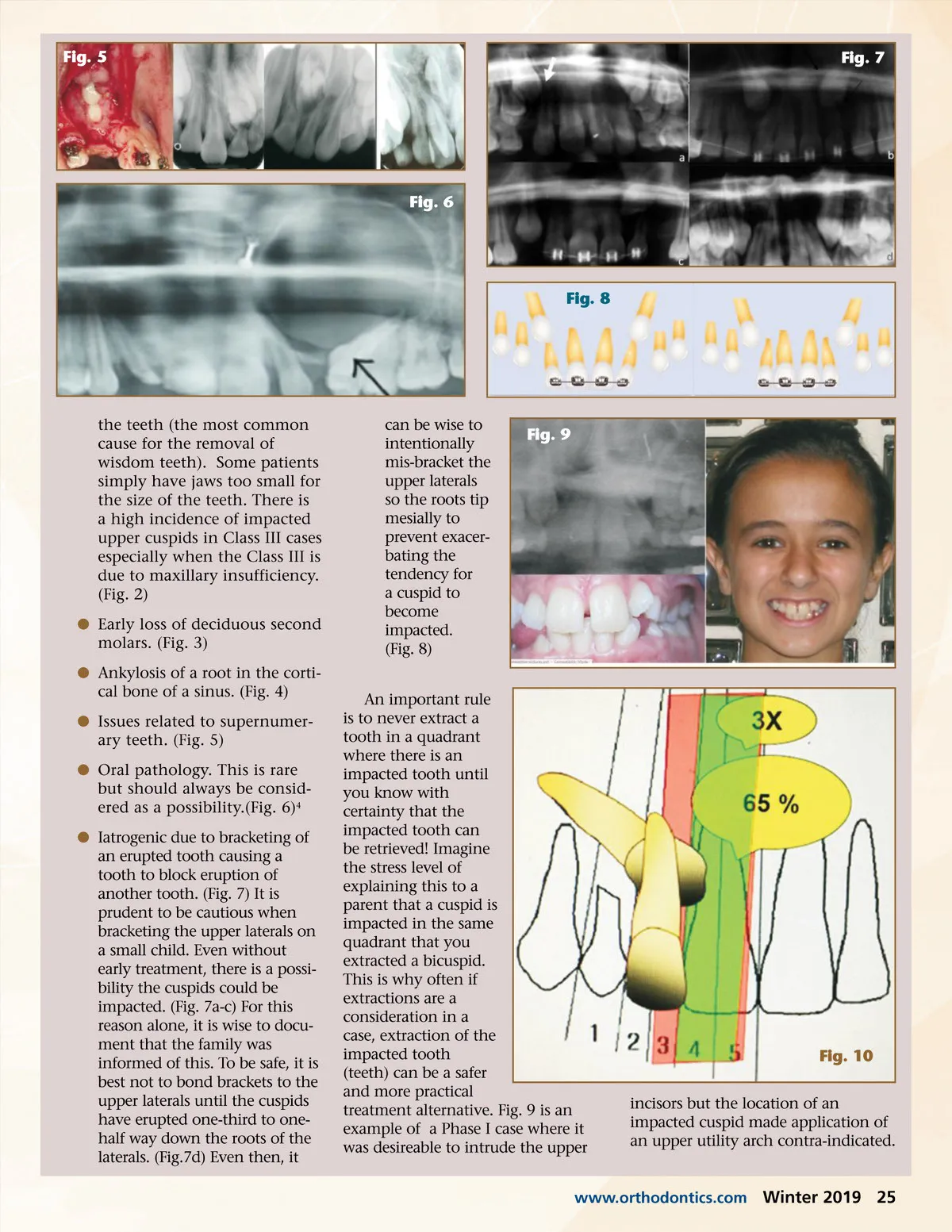
Fig. 5 Fig. 7 Fig. 6 Fig. 8 the teeth (the most common cause for the removal of wisdom teeth). Some patients simply have jaws too small for the size of the teeth. There is a high incidence of impacted upper cuspids in Class III cases especially when the Class III is due to maxillary insufficiency. (Fig. 2) b Early loss of deciduous second molars. (Fig. 3) b Ankylosis of a root in the corti-cal bone of a sinus. (Fig. 4) b Issues related to supernumer-ary teeth. (Fig. 5) b Oral pathology. This is rare but should always be consid-ered as a possibility.(Fig. 6) 4 b Iatrogenic due to bracketing of an erupted tooth causing a tooth to block eruption of another tooth. (Fig. 7) It is prudent to be cautious when bracketing the upper laterals on a small child. Even without early treatment, there is a possi-bility the cuspids could be impacted. (Fig. 7a-c) For this reason alone, it is wise to docu-ment that the family was informed of this. To be safe, it is best not to bond brackets to the upper laterals until the cuspids have erupted one-third to one-half way down the roots of the laterals. (Fig.7d) Even then, it can be wise to intentionally mis-bracket the upper laterals so the roots tip mesially to prevent exacer-bating the tendency for a cuspid to become impacted. (Fig. 8) Fig. 9 An important rule is to never extract a tooth in a quadrant where there is an impacted tooth until you know with certainty that the impacted tooth can be retrieved! Imagine the stress level of explaining this to a parent that a cuspid is impacted in the same quadrant that you extracted a bicuspid. This is why often if extractions are a consideration in a case, extraction of the impacted tooth (teeth) can be a safer and more practical treatment alternative. Fig. 9 is an example of a Phase I case where it was desireable to intrude the upper Fig. 10 incisors but the location of an impacted cuspid made application of an upper utility arch contra-indicated. www.orthodontics.com Winter 2019 25
Journal of the American Orthodontic Society Winter 2019: Page 25