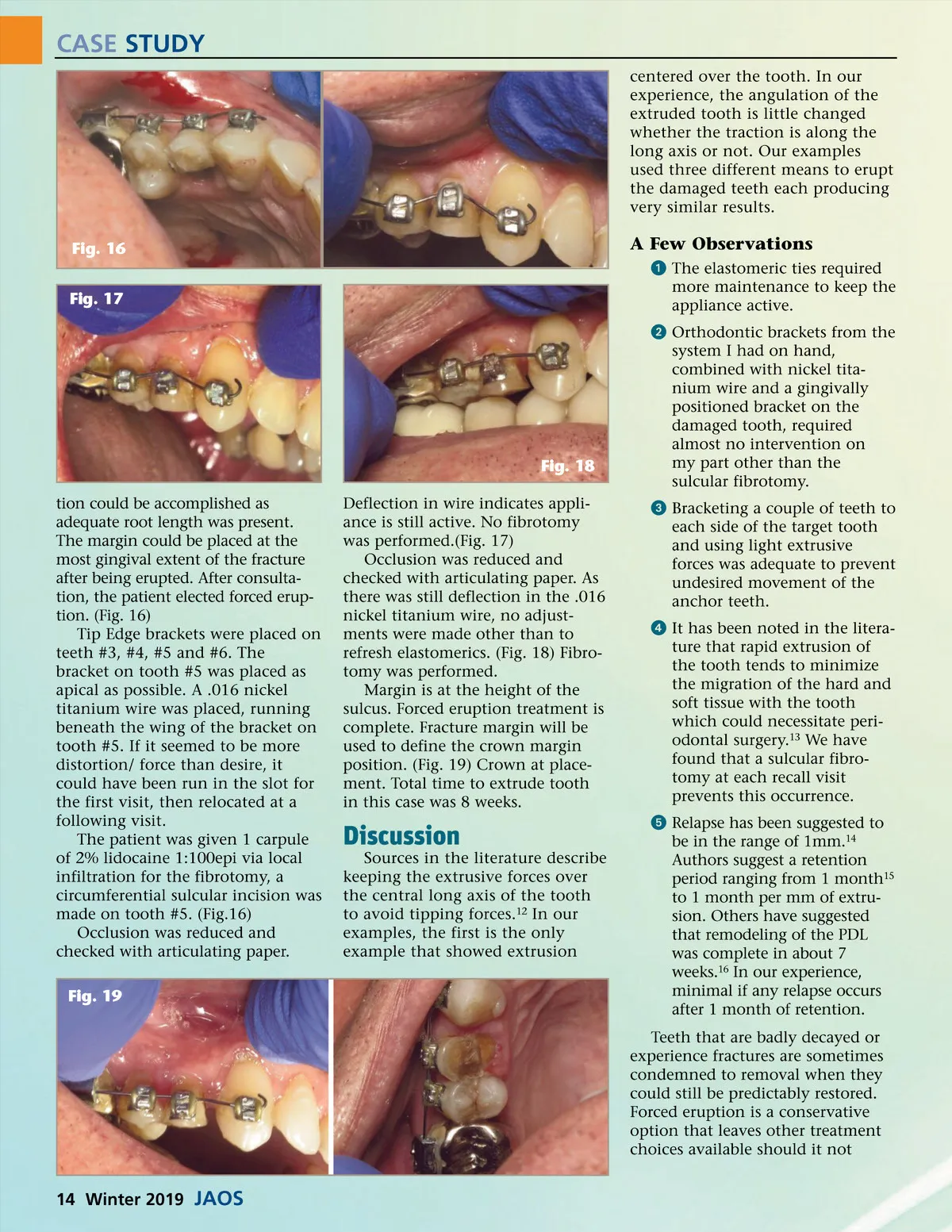
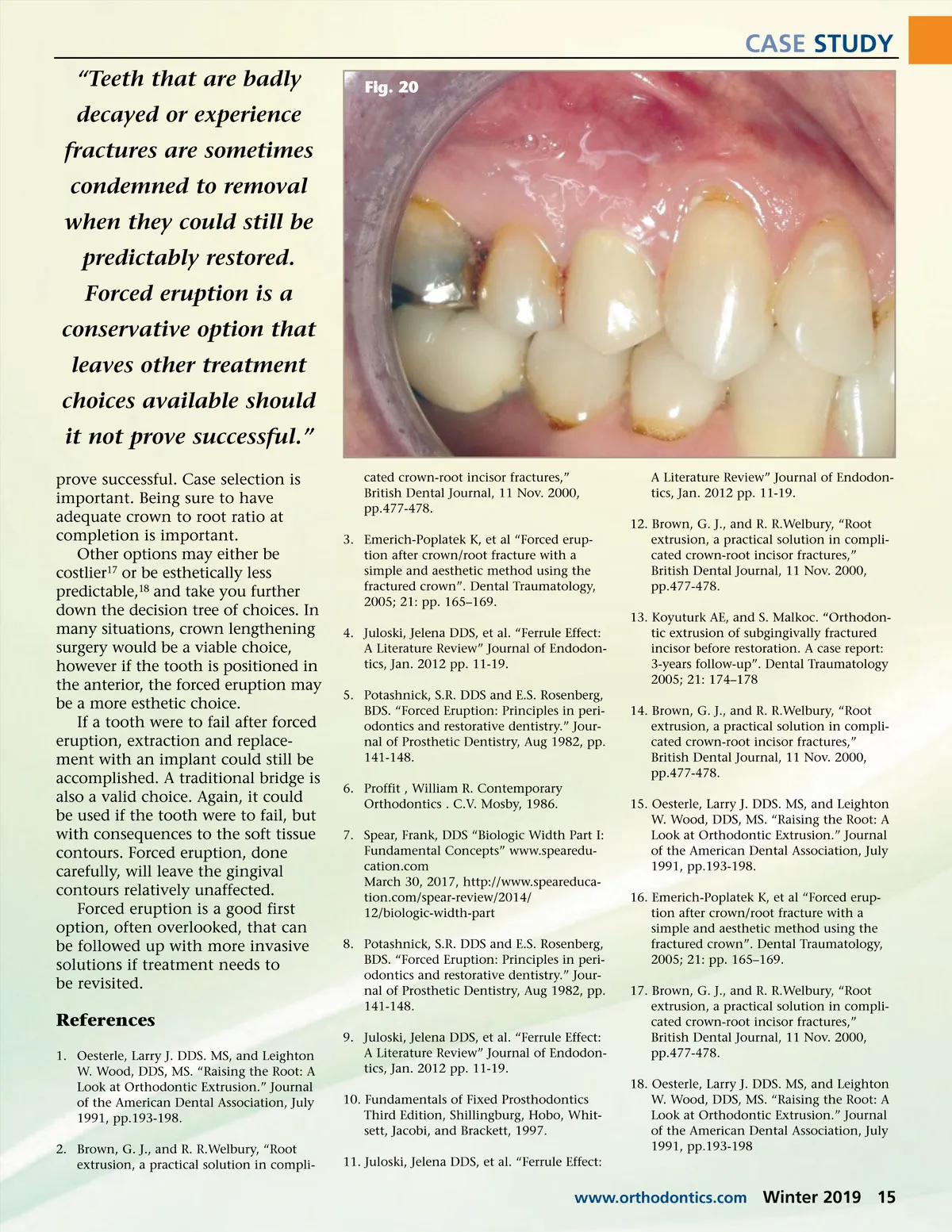
CASE STUDY centered over the tooth. In our experience, the angulation of the extruded tooth is little changed whether the traction is along the long axis or not. Our examples used three different means to erupt the damaged teeth each producing very similar results. Fig. 16 Fig. 17 A Few Observations ᕡ The elastomeric ties required more maintenance to keep the appliance active. ᕢ Orthodontic brackets from the system I had on hand, combined with nickel tita-nium wire and a gingivally positioned bracket on the damaged tooth, required almost no intervention on my part other than the sulcular fibrotomy. ᕣ Bracketing a couple of teeth to each side of the target tooth and using light extrusive forces was adequate to prevent undesired movement of the anchor teeth. ᕤ It has been noted in the litera-ture that rapid extrusion of the tooth tends to minimize the migration of the hard and soft tissue with the tooth which could necessitate peri-odontal surgery. 13 We have found that a sulcular fibro-tomy at each recall visit prevents this occurrence. ᕥ Relapse has been suggested to be in the range of 1mm. 14 Authors suggest a retention period ranging from 1 month 15 to 1 month per mm of extru-sion. Others have suggested that remodeling of the PDL was complete in about 7 weeks. 16 In our experience, minimal if any relapse occurs after 1 month of retention. Teeth that are badly decayed or experience fractures are sometimes condemned to removal when they could still be predictably restored. Forced eruption is a conservative option that leaves other treatment choices available should it not Fig. 18 tion could be accomplished as adequate root length was present. The margin could be placed at the most gingival extent of the fracture after being erupted. After consulta-tion, the patient elected forced erup-tion. (Fig. 16) Tip Edge brackets were placed on teeth #3, #4, #5 and #6. The bracket on tooth #5 was placed as apical as possible. A .016 nickel titanium wire was placed, running beneath the wing of the bracket on tooth #5. If it seemed to be more distortion/ force than desire, it could have been run in the slot for the first visit, then relocated at a following visit. The patient was given 1 carpule of 2% lidocaine 1:100epi via local infiltration for the fibrotomy, a circumferential sulcular incision was made on tooth #5. (Fig.16) Occlusion was reduced and checked with articulating paper. Fig. 19 Deflection in wire indicates appli-ance is still active. No fibrotomy was performed.(Fig. 17) Occlusion was reduced and checked with articulating paper. As there was still deflection in the .016 nickel titanium wire, no adjust-ments were made other than to refresh elastomerics. (Fig. 18) Fibro-tomy was performed. Margin is at the height of the sulcus. Forced eruption treatment is complete. Fracture margin will be used to define the crown margin position. (Fig. 19) Crown at place-ment. Total time to extrude tooth in this case was 8 weeks. Discussion Sources in the literature describe keeping the extrusive forces over the central long axis of the tooth to avoid tipping forces. 12 In our examples, the first is the only example that showed extrusion 14 Winter 2019 JAOS
Journal of the American Orthodontic Society Winter 2019: Page 14