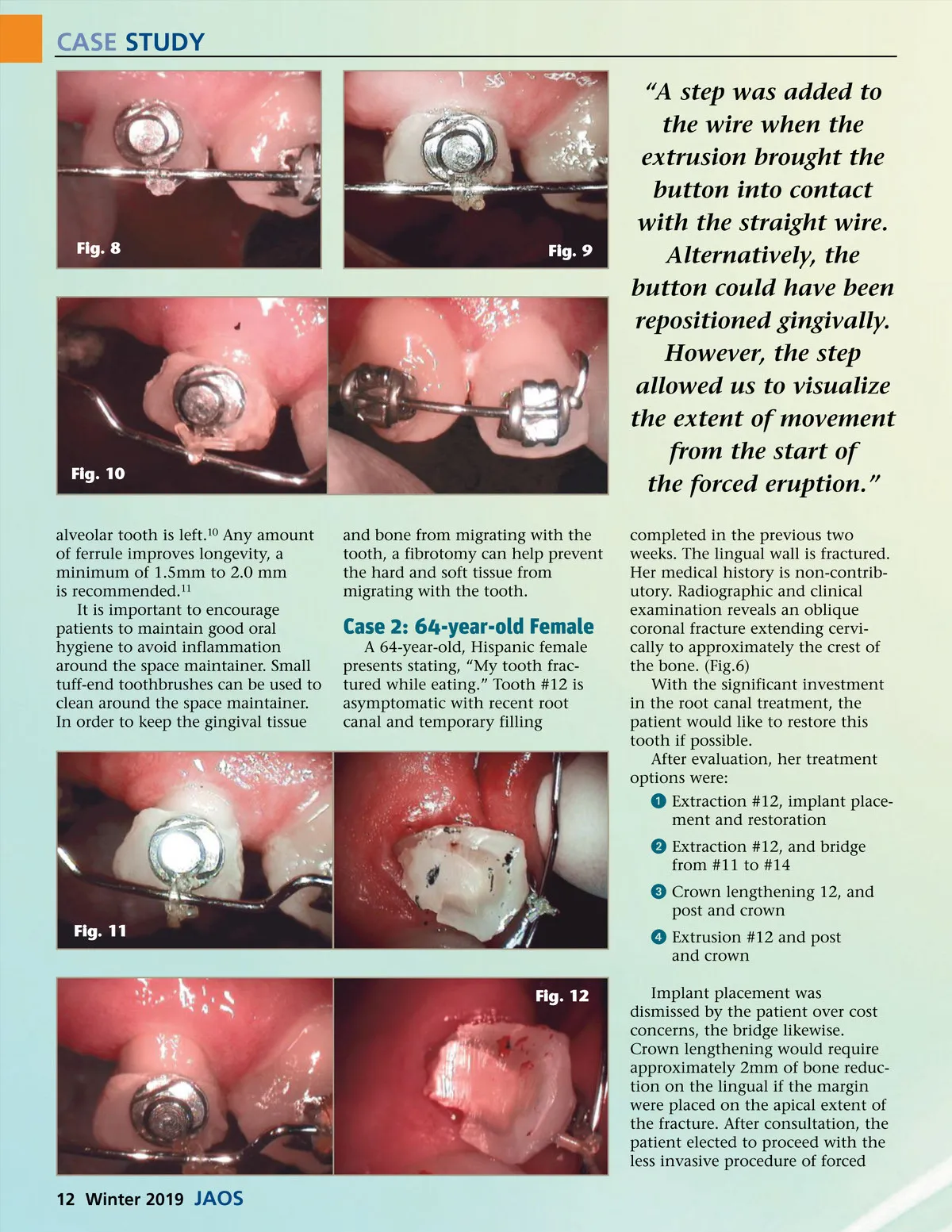
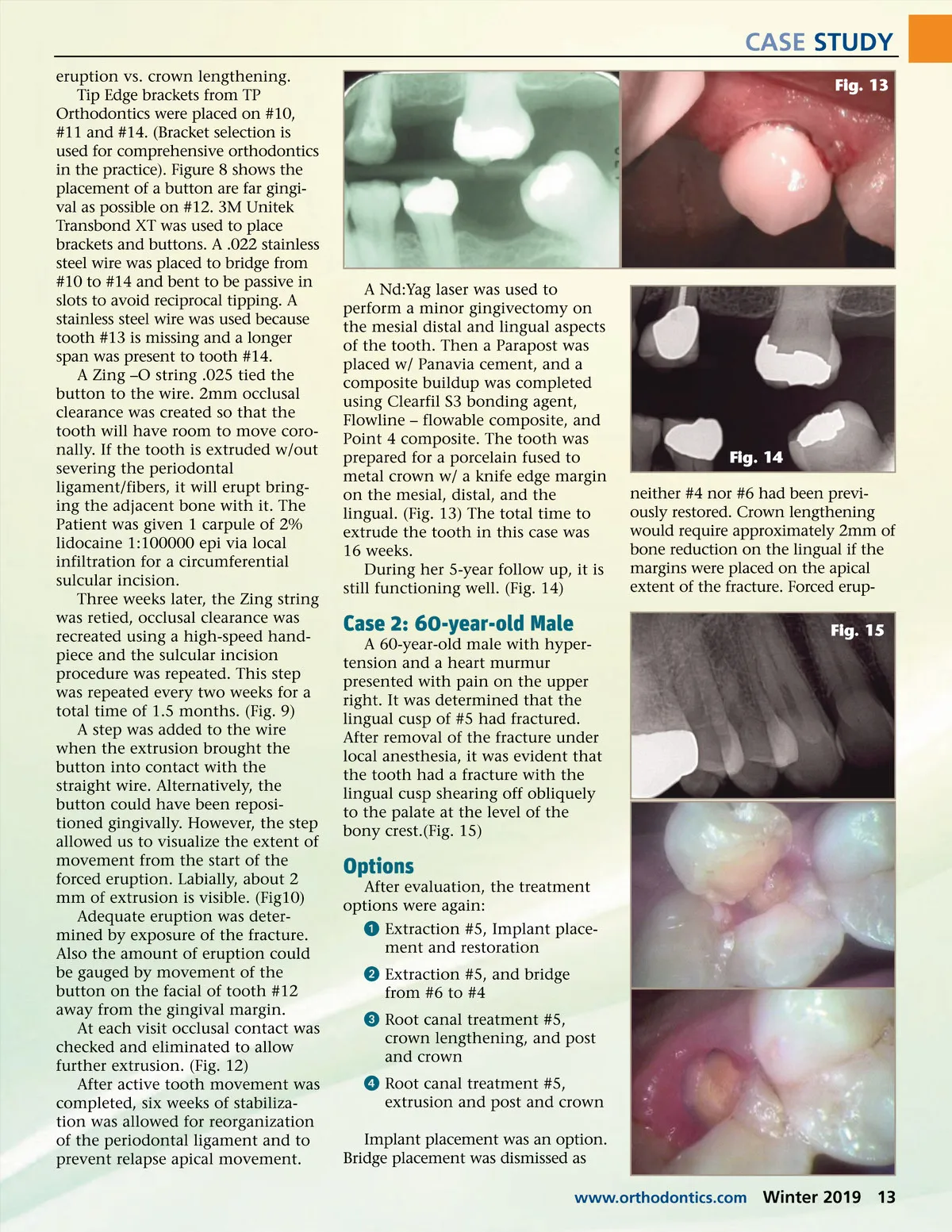
CASE STUDY eruption vs. crown lengthening. Tip Edge brackets from TP Orthodontics were placed on #10, #11 and #14. (Bracket selection is used for comprehensive orthodontics in the practice). Figure 8 shows the placement of a button are far gingi-val as possible on #12. 3M Unitek Transbond XT was used to place brackets and buttons. A .022 stainless steel wire was placed to bridge from #10 to #14 and bent to be passive in slots to avoid reciprocal tipping. A stainless steel wire was used because tooth #13 is missing and a longer span was present to tooth #14. A Zing –O string .025 tied the button to the wire. 2mm occlusal clearance was created so that the tooth will have room to move coro-nally. If the tooth is extruded w/out severing the periodontal ligament/fibers, it will erupt bring-ing the adjacent bone with it. The Patient was given 1 carpule of 2% lidocaine 1:100000 epi via local infiltration for a circumferential sulcular incision. Three weeks later, the Zing string was retied, occlusal clearance was recreated using a high-speed hand-piece and the sulcular incision procedure was repeated. This step was repeated every two weeks for a total time of 1.5 months. (Fig. 9) A step was added to the wire when the extrusion brought the button into contact with the straight wire. Alternatively, the button could have been reposi-tioned gingivally. However, the step allowed us to visualize the extent of movement from the start of the forced eruption. Labially, about 2 mm of extrusion is visible. (Fig10) Adequate eruption was deter-mined by exposure of the fracture. Also the amount of eruption could be gauged by movement of the button on the facial of tooth #12 away from the gingival margin. At each visit occlusal contact was checked and eliminated to allow further extrusion. (Fig. 12) After active tooth movement was completed, six weeks of stabiliza-tion was allowed for reorganization of the periodontal ligament and to prevent relapse apical movement. Fig. 13 A Nd:Yag laser was used to perform a minor gingivectomy on the mesial distal and lingual aspects of the tooth. Then a Parapost was placed w/ Panavia cement, and a composite buildup was completed using Clearfil S3 bonding agent, Flowline – flowable composite, and Point 4 composite. The tooth was prepared for a porcelain fused to metal crown w/ a knife edge margin on the mesial, distal, and the lingual. (Fig. 13) The total time to extrude the tooth in this case was 16 weeks. During her 5-year follow up, it is still functioning well. (Fig. 14) Fig. 14 neither #4 nor #6 had been previ-ously restored. Crown lengthening would require approximately 2mm of bone reduction on the lingual if the margins were placed on the apical extent of the fracture. Forced erup-Fig. 15 Case 2: 60-year-old Male A 60-year-old male with hyper-tension and a heart murmur presented with pain on the upper right. It was determined that the lingual cusp of #5 had fractured. After removal of the fracture under local anesthesia, it was evident that the tooth had a fracture with the lingual cusp shearing off obliquely to the palate at the level of the bony crest.(Fig. 15) Options After evaluation, the treatment options were again: ᕡ Extraction #5, Implant place-ment and restoration ᕢ Extraction #5, and bridge from #6 to #4 ᕣ Root canal treatment #5, crown lengthening, and post and crown ᕤ Root canal treatment #5, extrusion and post and crown Implant placement was an option. Bridge placement was dismissed as www.orthodontics.com Winter 2019 13
Journal of the American Orthodontic Society Winter 2019: Page 13