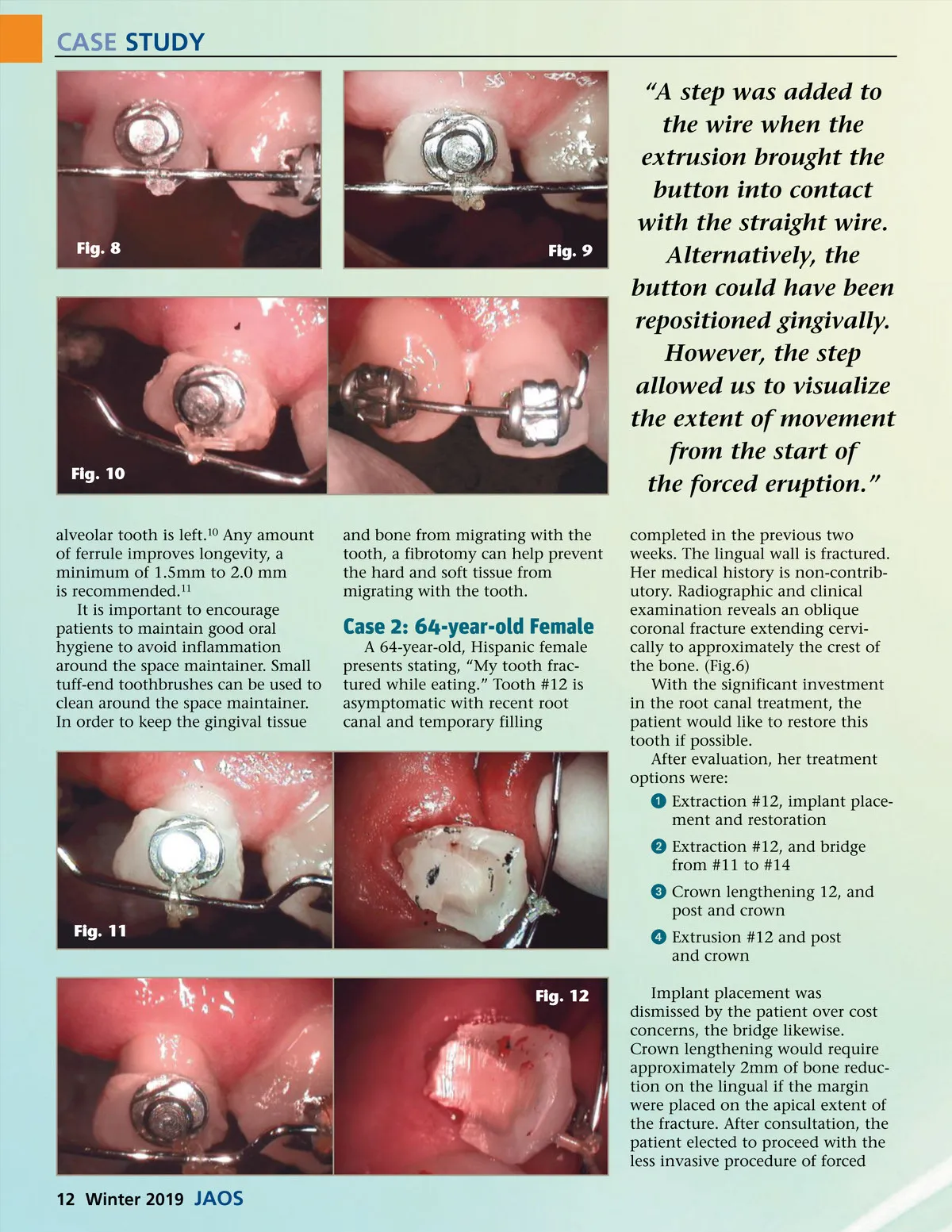
CASE STUDY “A step was added to the wire when the extrusion brought the button into contact with the straight wire. Alternatively, the button could have been repositioned gingivally. However, the step allowed us to visualize the extent of movement from the start of the forced eruption.” completed in the previous two weeks. The lingual wall is fractured. Her medical history is non-contrib-utory. Radiographic and clinical examination reveals an oblique coronal fracture extending cervi-cally to approximately the crest of the bone. (Fig.6) With the significant investment in the root canal treatment, the patient would like to restore this tooth if possible. After evaluation, her treatment options were: ᕡ Extraction #12, implant place-ment and restoration ᕢ Extraction #12, and bridge from #11 to #14 ᕣ Crown lengthening 12, and post and crown Fig. 11 ᕤ Extrusion #12 and post and crown Fig. 12 Implant placement was dismissed by the patient over cost concerns, the bridge likewise. Crown lengthening would require approximately 2mm of bone reduc-tion on the lingual if the margin were placed on the apical extent of the fracture. After consultation, the patient elected to proceed with the less invasive procedure of forced Fig. 8 Fig. 9 Fig. 10 alveolar tooth is left. 10 Any amount of ferrule improves longevity, a minimum of 1.5mm to 2.0 mm is recommended. 11 It is important to encourage patients to maintain good oral hygiene to avoid inflammation around the space maintainer. Small tuff-end toothbrushes can be used to clean around the space maintainer. In order to keep the gingival tissue and bone from migrating with the tooth, a fibrotomy can help prevent the hard and soft tissue from migrating with the tooth. Case 2: 64-year-old Female A 64-year-old, Hispanic female presents stating, “My tooth frac-tured while eating.” Tooth #12 is asymptomatic with recent root canal and temporary filling 12 Winter 2019 JAOS
Journal of the American Orthodontic Society Winter 2019: Page 12