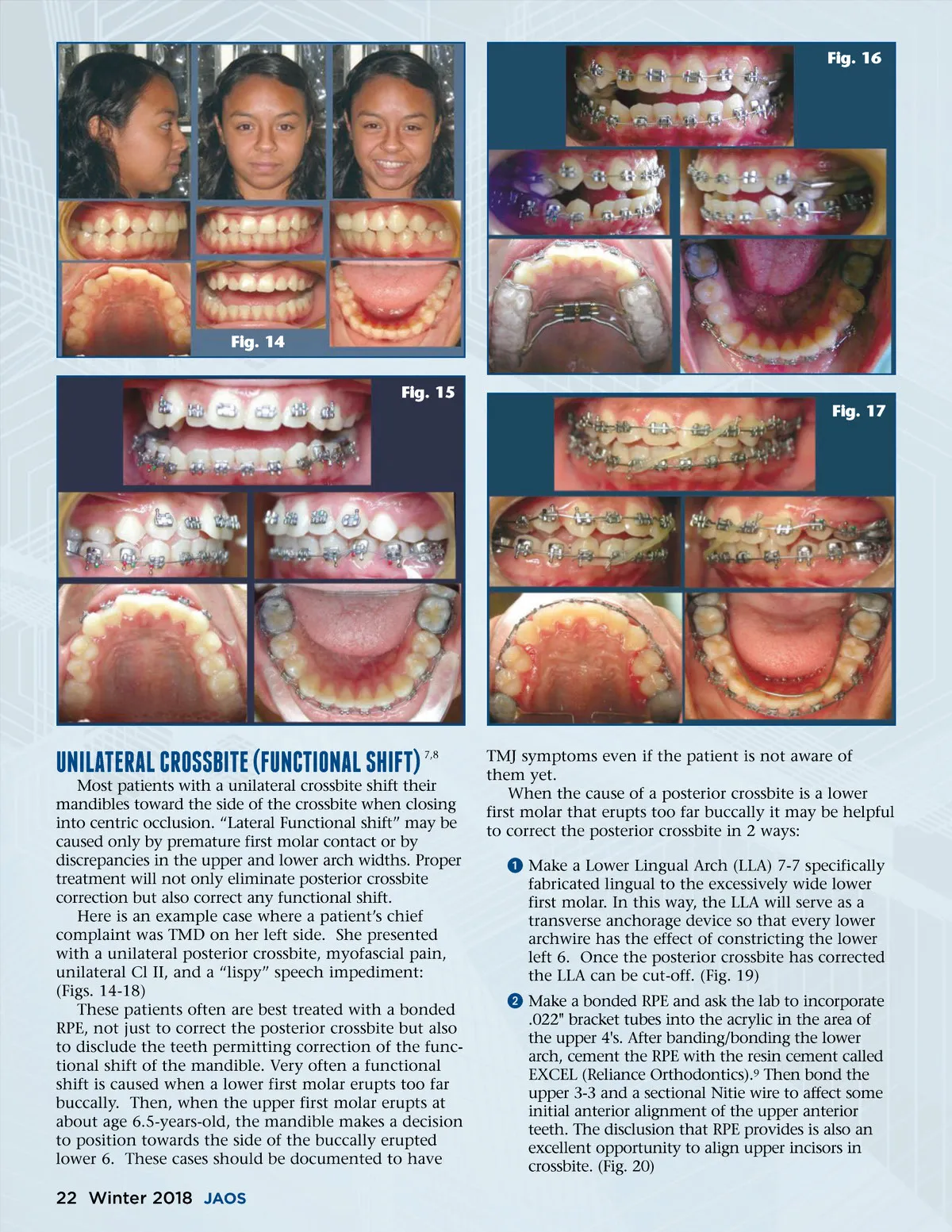
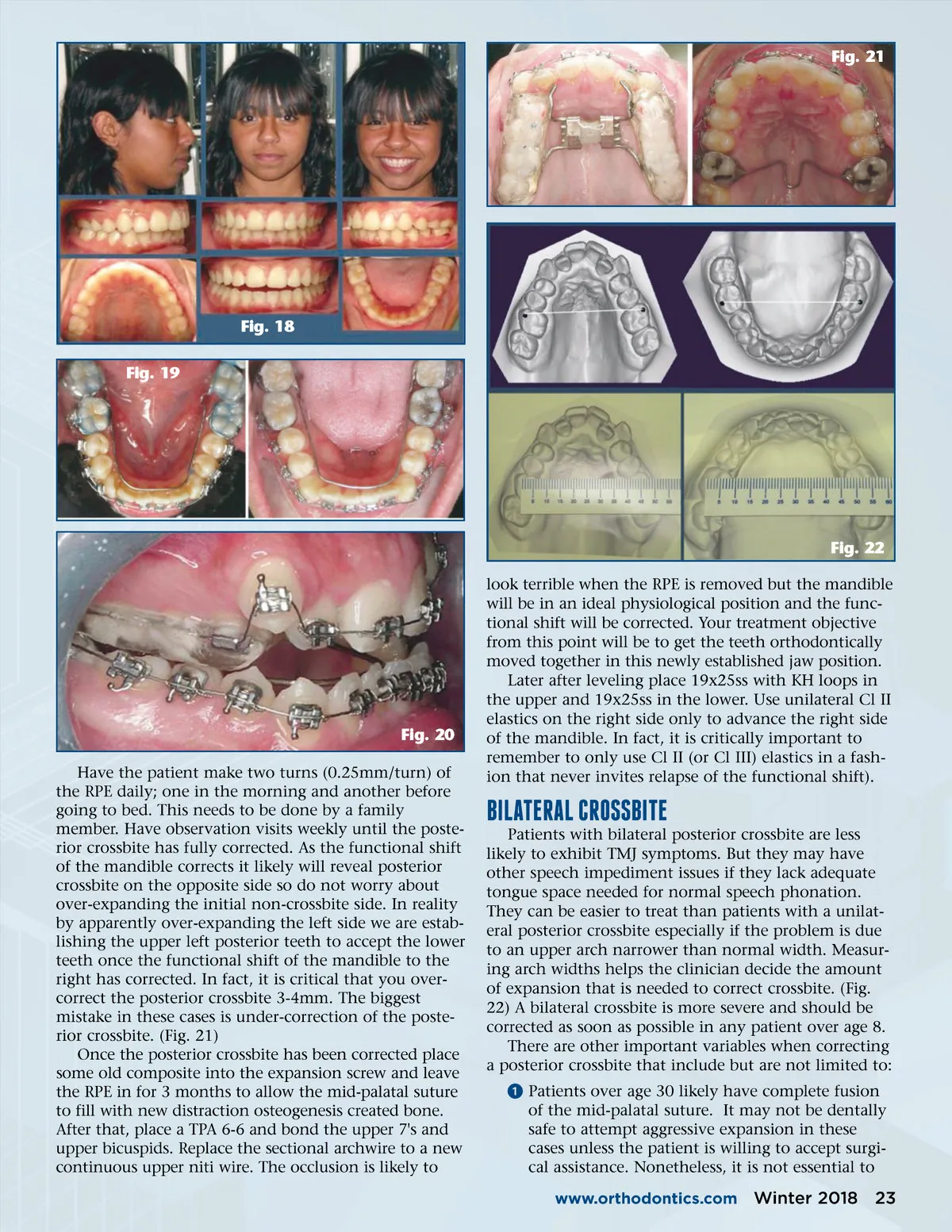
Fig. 21 Fig. 18 Fig. 19 Fig. 22 look terrible when the RPE is removed but the mandible will be in an ideal physiological position and the func-tional shift will be corrected. Your treatment objective from this point will be to get the teeth orthodontically moved together in this newly established jaw position. Later after leveling place 19x25ss with KH loops in the upper and 19x25ss in the lower. Use unilateral Cl II elastics on the right side only to advance the right side of the mandible. In fact, it is critically important to remember to only use Cl II (or Cl III) elastics in a fash-ion that never invites relapse of the functional shift). Fig. 20 Have the patient make two turns (0.25mm/turn) of the RPE daily; one in the morning and another before going to bed. This needs to be done by a family member. Have observation visits weekly until the poste-rior crossbite has fully corrected. As the functional shift of the mandible corrects it likely will reveal posterior crossbite on the opposite side so do not worry about over-expanding the initial non-crossbite side. In reality by apparently over-expanding the left side we are estab-lishing the upper left posterior teeth to accept the lower teeth once the functional shift of the mandible to the right has corrected. In fact, it is critical that you over-correct the posterior crossbite 3-4mm. The biggest mistake in these cases is under-correction of the poste-rior crossbite. (Fig. 21) Once the posterior crossbite has been corrected place some old composite into the expansion screw and leave the RPE in for 3 months to allow the mid-palatal suture to fill with new distraction osteogenesis created bone. After that, place a TPA 6-6 and bond the upper 7's and upper bicuspids. Replace the sectional archwire to a new continuous upper niti wire. The occlusion is likely to bIlATERAl CRossbITE Patients with bilateral posterior crossbite are less likely to exhibit TMJ symptoms. But they may have other speech impediment issues if they lack adequate tongue space needed for normal speech phonation. They can be easier to treat than patients with a unilat-eral posterior crossbite especially if the problem is due to an upper arch narrower than normal width. Measur-ing arch widths helps the clinician decide the amount of expansion that is needed to correct crossbite. (Fig. 22) A bilateral crossbite is more severe and should be corrected as soon as possible in any patient over age 8. There are other important variables when correcting a posterior crossbite that include but are not limited to: ᕡ Patients over age 30 likely have complete fusion of the mid-palatal suture. It may not be dentally safe to attempt aggressive expansion in these cases unless the patient is willing to accept surgi-cal assistance. Nonetheless, it is not essential to www.orthodontics.com Winter 2018 23
Journal of the American Orthodontic Society Winter 2018: Page 23