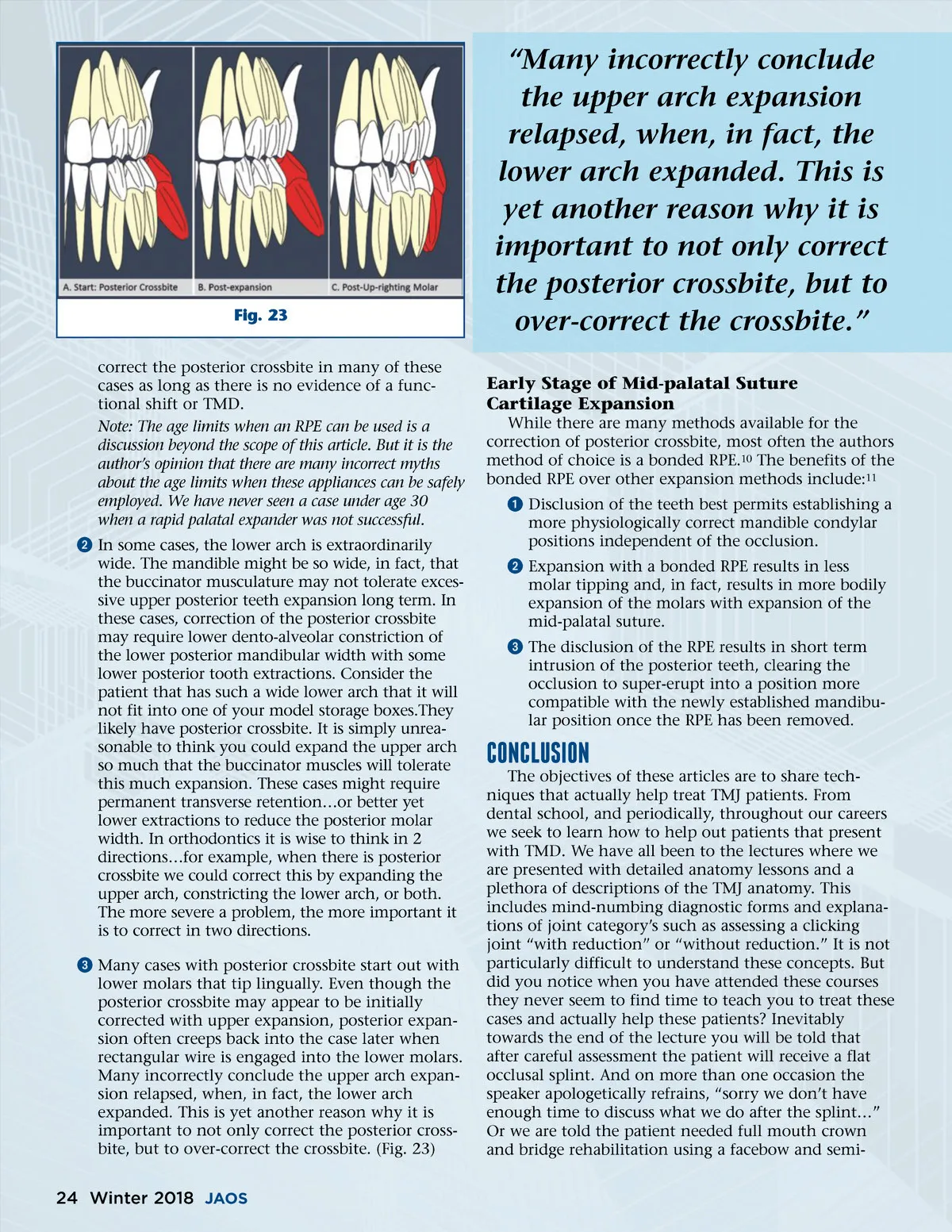
Fig. 23 correct the posterior crossbite in many of these cases as long as there is no evidence of a func-tional shift or TMD. Note: The age limits when an RPE can be used is a discussion beyond the scope of this article. But it is the author’s opinion that there are many incorrect myths about the age limits when these appliances can be safely employed. We have never seen a case under age 30 when a rapid palatal expander was not successful. ᕢ In some cases, the lower arch is extraordinarily wide. The mandible might be so wide, in fact, that the buccinator musculature may not tolerate exces-sive upper posterior teeth expansion long term. In these cases, correction of the posterior crossbite may require lower dento-alveolar constriction of the lower posterior mandibular width with some lower posterior tooth extractions. Consider the patient that has such a wide lower arch that it will not fit into one of your model storage boxes.They likely have posterior crossbite. It is simply unrea-sonable to think you could expand the upper arch so much that the buccinator muscles will tolerate this much expansion. These cases might require permanent transverse retention…or better yet lower extractions to reduce the posterior molar width. In orthodontics it is wise to think in 2 directions…for example, when there is posterior crossbite we could correct this by expanding the upper arch, constricting the lower arch, or both. The more severe a problem, the more important it is to correct in two directions. ᕣ Many cases with posterior crossbite start out with lower molars that tip lingually. Even though the posterior crossbite may appear to be initially corrected with upper expansion, posterior expan-sion often creeps back into the case later when rectangular wire is engaged into the lower molars. Many incorrectly conclude the upper arch expan-sion relapsed, when, in fact, the lower arch expanded. This is yet another reason why it is important to not only correct the posterior cross-bite, but to over-correct the crossbite. (Fig. 23) “Many incorrectly conclude the upper arch expansion relapsed, when, in fact, the lower arch expanded. This is yet another reason why it is important to not only correct the posterior crossbite, but to over-correct the crossbite.” Early Stage of Mid-palatal Suture Cartilage Expansion While there are many methods available for the correction of posterior crossbite, most often the authors method of choice is a bonded RPE. 10 The benefits of the bonded RPE over other expansion methods include: 11 ᕡ Disclusion of the teeth best permits establishing a more physiologically correct mandible condylar positions independent of the occlusion. ᕢ Expansion with a bonded RPE results in less molar tipping and, in fact, results in more bodily expansion of the molars with expansion of the mid-palatal suture. ᕣ The disclusion of the RPE results in short term intrusion of the posterior teeth, clearing the occlusion to super-erupt into a position more compatible with the newly established mandibu-lar position once the RPE has been removed. The objectives of these articles are to share tech-niques that actually help treat TMJ patients. From dental school, and periodically, throughout our careers we seek to learn how to help out patients that present with TMD. We have all been to the lectures where we are presented with detailed anatomy lessons and a plethora of descriptions of the TMJ anatomy. This includes mind-numbing diagnostic forms and explana-tions of joint category’s such as assessing a clicking joint “with reduction” or “without reduction.” It is not particularly difficult to understand these concepts. But did you notice when you have attended these courses they never seem to find time to teach you to treat these cases and actually help these patients? Inevitably towards the end of the lecture you will be told that after careful assessment the patient will receive a flat occlusal splint. And on more than one occasion the speaker apologetically refrains, “sorry we don’t have enough time to discuss what we do after the splint…” Or we are told the patient needed full mouth crown and bridge rehabilitation using a facebow and semi-CoNClUsIoN 24 Winter 2018 JAOS
Journal of the American Orthodontic Society Winter 2018: Page 24