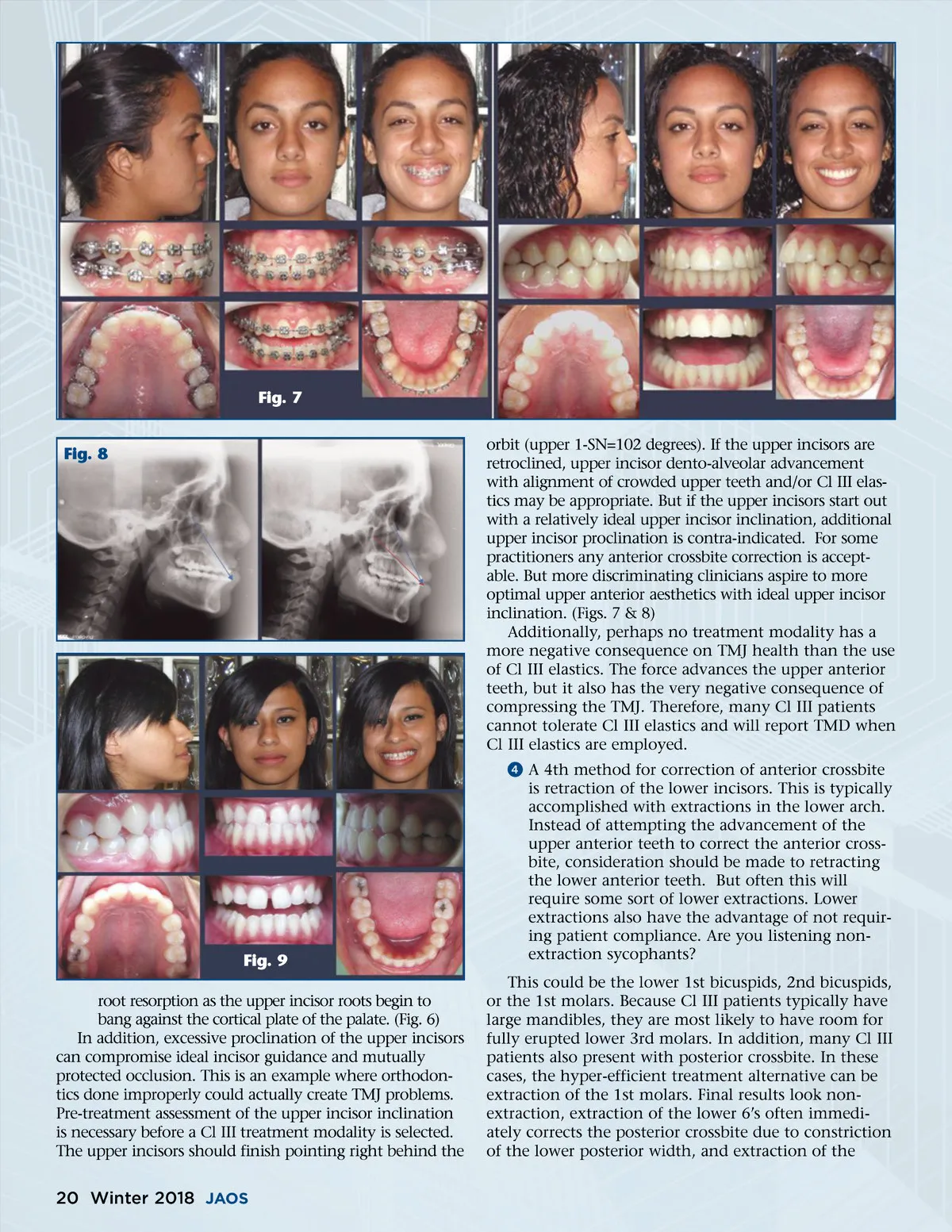
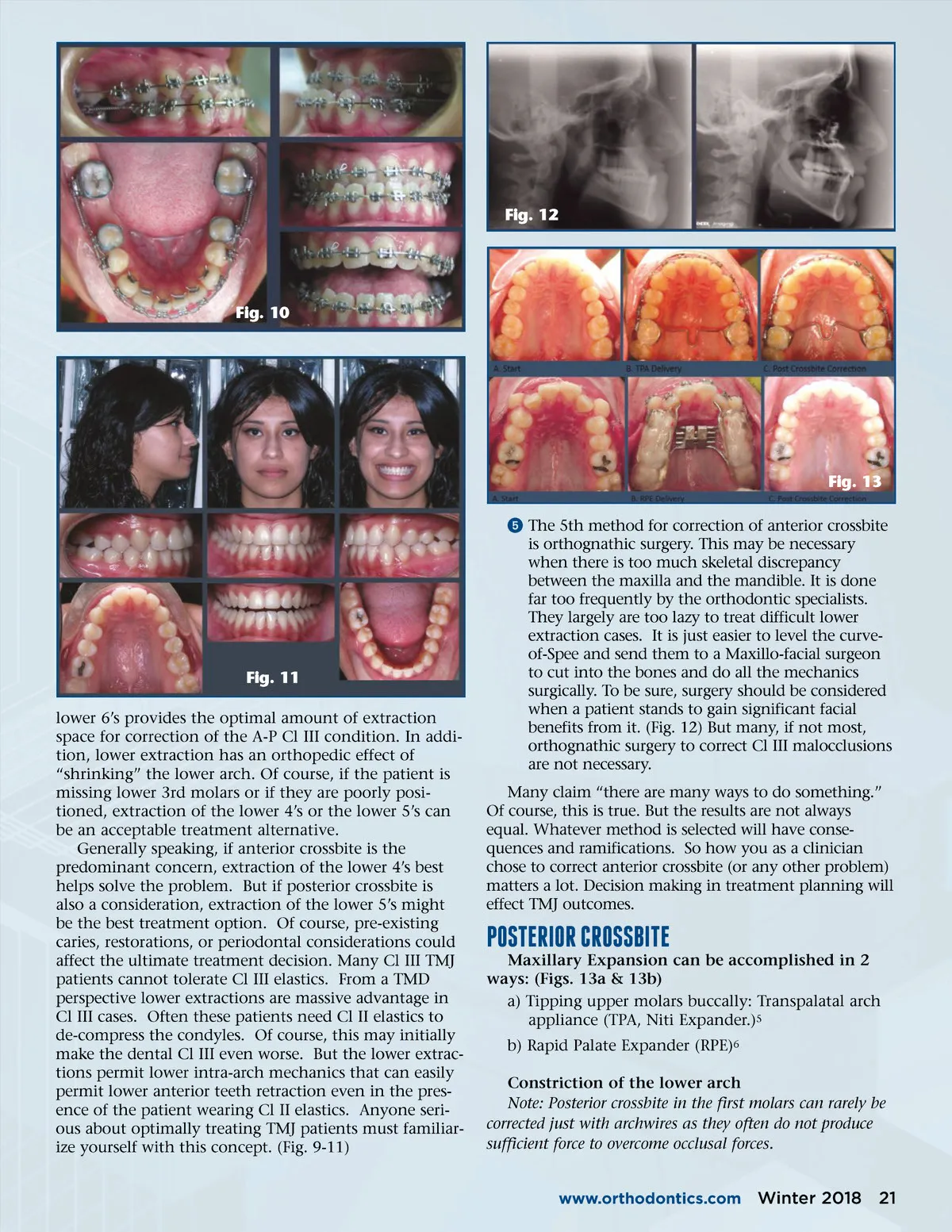
Fig. 12 Fig. 10 Fig. 13 ᕥ The 5th method for correction of anterior crossbite is orthognathic surgery. This may be necessary when there is too much skeletal discrepancy between the maxilla and the mandible. It is done far too frequently by the orthodontic specialists. They largely are too lazy to treat difficult lower extraction cases. It is just easier to level the curve-of-Spee and send them to a Maxillo-facial surgeon to cut into the bones and do all the mechanics surgically. To be sure, surgery should be considered when a patient stands to gain significant facial benefits from it. (Fig. 12) But many, if not most, orthognathic surgery to correct Cl III malocclusions are not necessary. Many claim “there are many ways to do something.” Of course, this is true. But the results are not always equal. Whatever method is selected will have conse-quences and ramifications. So how you as a clinician chose to correct anterior crossbite (or any other problem) matters a lot. Decision making in treatment planning will effect TMJ outcomes. Fig. 11 lower 6’s provides the optimal amount of extraction space for correction of the A-P Cl III condition. In addi-tion, lower extraction has an orthopedic effect of “shrinking” the lower arch. Of course, if the patient is missing lower 3rd molars or if they are poorly posi-tioned, extraction of the lower 4’s or the lower 5’s can be an acceptable treatment alternative. Generally speaking, if anterior crossbite is the predominant concern, extraction of the lower 4’s best helps solve the problem. But if posterior crossbite is also a consideration, extraction of the lower 5’s might be the best treatment option. Of course, pre-existing caries, restorations, or periodontal considerations could affect the ultimate treatment decision. Many Cl III TMJ patients cannot tolerate Cl III elastics. From a TMD perspective lower extractions are massive advantage in Cl III cases. Often these patients need Cl II elastics to de-compress the condyles. Of course, this may initially make the dental Cl III even worse. But the lower extrac-tions permit lower intra-arch mechanics that can easily permit lower anterior teeth retraction even in the pres-ence of the patient wearing Cl II elastics. Anyone seri-ous about optimally treating TMJ patients must familiar-ize yourself with this concept. (Fig. 9-11) Maxillary Expansion can be accomplished in 2 ways: (Figs. 13a & 13b) a) Tipping upper molars buccally: Transpalatal arch appliance (TPA, Niti Expander.) 5 b) Rapid Palate Expander (RPE) 6 Constriction of the lower arch Note: Posterior crossbite in the first molars can rarely be corrected just with archwires as they often do not produce sufficient force to overcome occlusal forces. PosTERIoR CRossbITE www.orthodontics.com Winter 2018 21
Journal of the American Orthodontic Society Winter 2018: Page 21