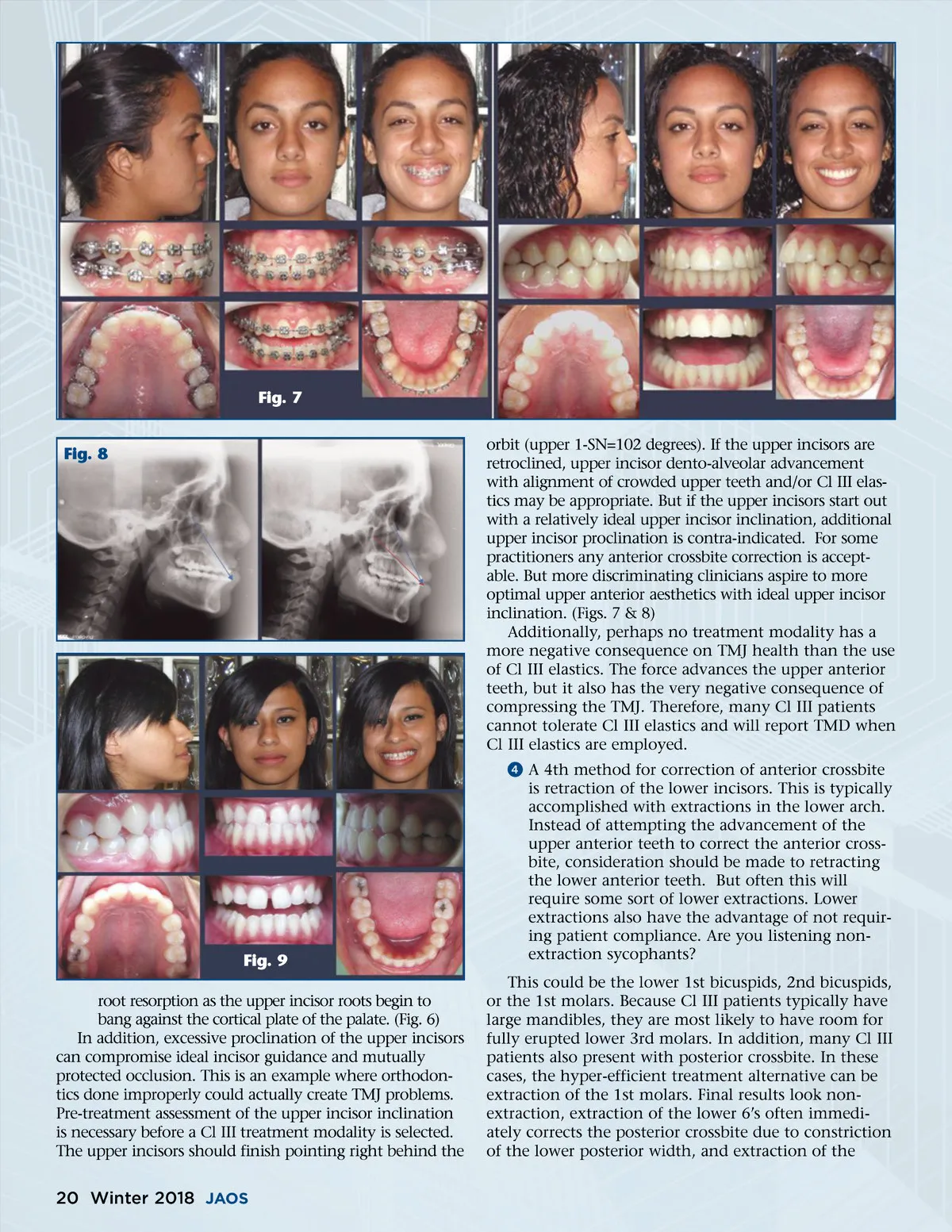
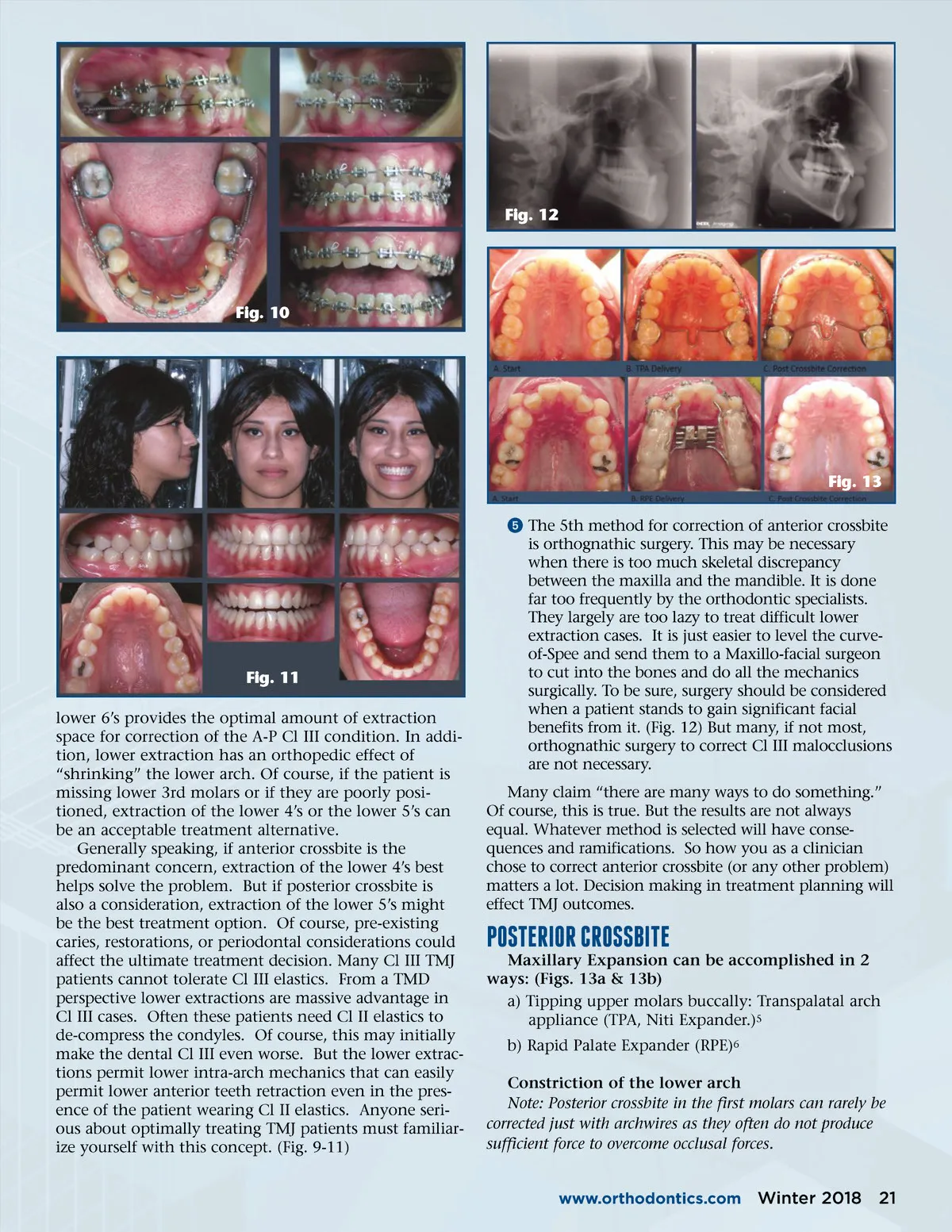
Fig. 7 orbit (upper 1-SN=102 degrees). If the upper incisors are retroclined, upper incisor dento-alveolar advancement with alignment of crowded upper teeth and/or Cl III elas-tics may be appropriate. But if the upper incisors start out with a relatively ideal upper incisor inclination, additional upper incisor proclination is contra-indicated. For some practitioners any anterior crossbite correction is accept-able. But more discriminating clinicians aspire to more optimal upper anterior aesthetics with ideal upper incisor inclination. (Figs. 7 & 8) Additionally, perhaps no treatment modality has a more negative consequence on TMJ health than the use of Cl III elastics. The force advances the upper anterior teeth, but it also has the very negative consequence of compressing the TMJ. Therefore, many Cl III patients cannot tolerate Cl III elastics and will report TMD when Cl III elastics are employed. ᕤ A 4th method for correction of anterior crossbite is retraction of the lower incisors. This is typically accomplished with extractions in the lower arch. Instead of attempting the advancement of the upper anterior teeth to correct the anterior cross-bite, consideration should be made to retracting the lower anterior teeth. But often this will require some sort of lower extractions. Lower extractions also have the advantage of not requir-ing patient compliance. Are you listening non-extraction sycophants? This could be the lower 1st bicuspids, 2nd bicuspids, or the 1st molars. Because Cl III patients typically have large mandibles, they are most likely to have room for fully erupted lower 3rd molars. In addition, many Cl III patients also present with posterior crossbite. In these cases, the hyper-efficient treatment alternative can be extraction of the 1st molars. Final results look non-extraction, extraction of the lower 6’s often immedi-ately corrects the posterior crossbite due to constriction of the lower posterior width, and extraction of the Fig. 8 Fig. 9 root resorption as the upper incisor roots begin to bang against the cortical plate of the palate. (Fig. 6) In addition, excessive proclination of the upper incisors can compromise ideal incisor guidance and mutually protected occlusion. This is an example where orthodon-tics done improperly could actually create TMJ problems. Pre-treatment assessment of the upper incisor inclination is necessary before a Cl III treatment modality is selected. The upper incisors should finish pointing right behind the 20 Winter 2018 JAOS
Journal of the American Orthodontic Society Winter 2018: Page 20