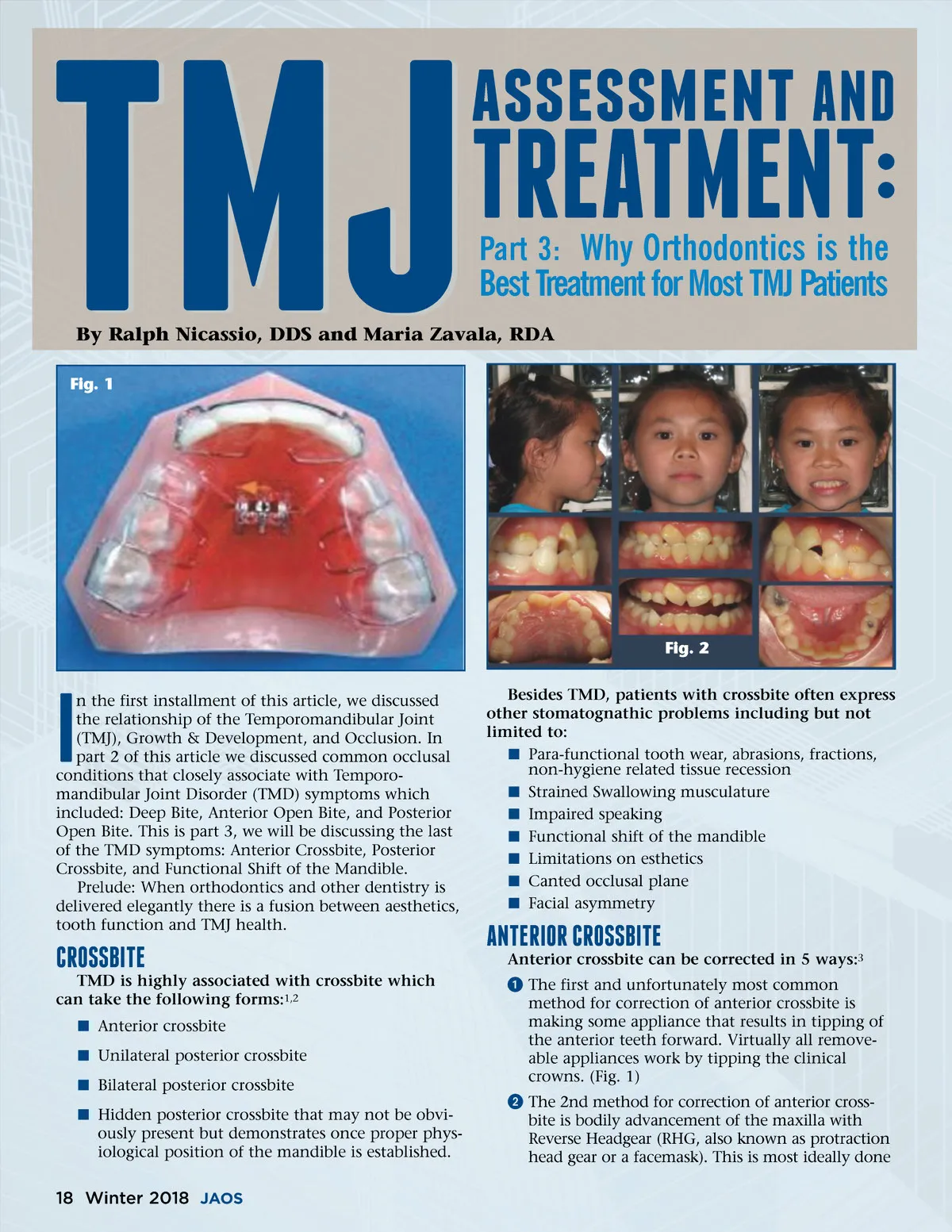
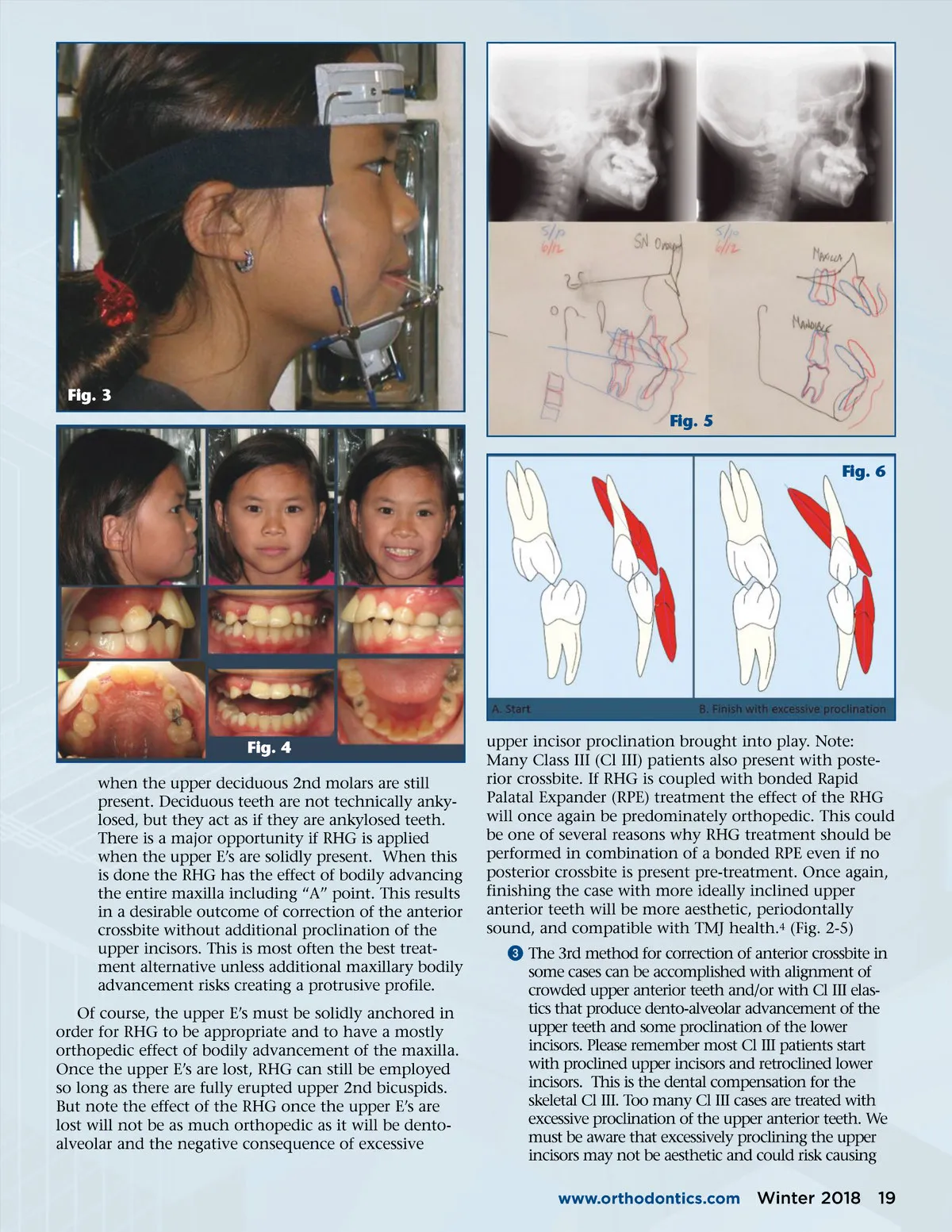
Fig. 3 Fig. 5 Fig. 6 Fig. 4 when the upper deciduous 2nd molars are still present. Deciduous teeth are not technically anky-losed, but they act as if they are ankylosed teeth. There is a major opportunity if RHG is applied when the upper E’s are solidly present. When this is done the RHG has the effect of bodily advancing the entire maxilla including “A” point. This results in a desirable outcome of correction of the anterior crossbite without additional proclination of the upper incisors. This is most often the best treat-ment alternative unless additional maxillary bodily advancement risks creating a protrusive profile. Of course, the upper E’s must be solidly anchored in order for RHG to be appropriate and to have a mostly orthopedic effect of bodily advancement of the maxilla. Once the upper E’s are lost, RHG can still be employed so long as there are fully erupted upper 2nd bicuspids. But note the effect of the RHG once the upper E’s are lost will not be as much orthopedic as it will be dento-alveolar and the negative consequence of excessive upper incisor proclination brought into play. Note: Many Class III (Cl III) patients also present with poste-rior crossbite. If RHG is coupled with bonded Rapid Palatal Expander (RPE) treatment the effect of the RHG will once again be predominately orthopedic. This could be one of several reasons why RHG treatment should be performed in combination of a bonded RPE even if no posterior crossbite is present pre-treatment. Once again, finishing the case with more ideally inclined upper anterior teeth will be more aesthetic, periodontally sound, and compatible with TMJ health. 4 (Fig. 2-5) ᕣ The 3rd method for correction of anterior crossbite in some cases can be accomplished with alignment of crowded upper anterior teeth and/or with Cl III elas-tics that produce dento-alveolar advancement of the upper teeth and some proclination of the lower incisors. Please remember most Cl III patients start with proclined upper incisors and retroclined lower incisors. This is the dental compensation for the skeletal Cl III. Too many Cl III cases are treated with excessive proclination of the upper anterior teeth. We must be aware that excessively proclining the upper incisors may not be aesthetic and could risk causing www.orthodontics.com Winter 2018 19
Journal of the American Orthodontic Society Winter 2018: Page 19