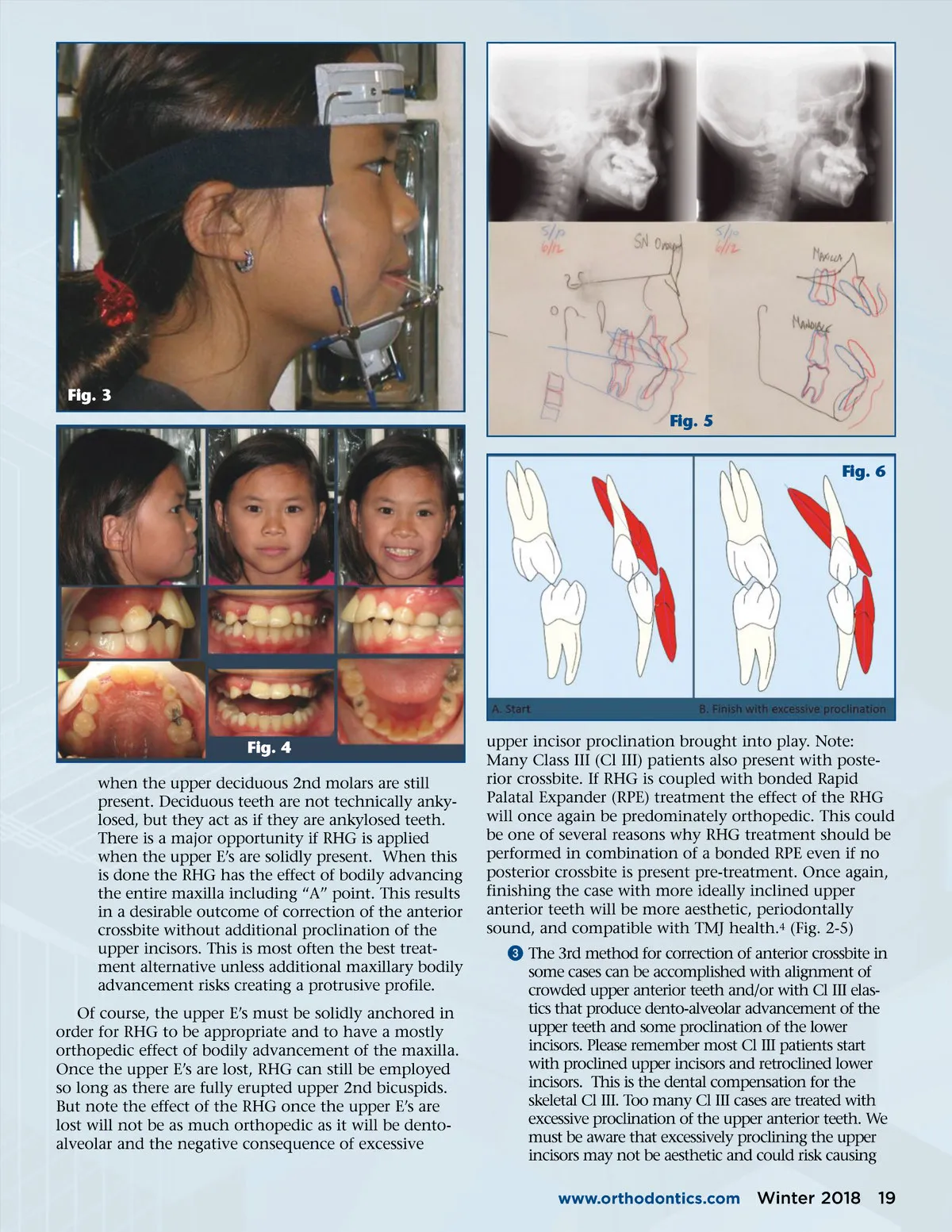
TMJ Fig. 1 n the first installment of this article, we discussed the relationship of the Temporomandibular Joint (TMJ), Growth & Development, and Occlusion. In part 2 of this article we discussed common occlusal conditions that closely associate with Temporo-mandibular Joint Disorder (TMD) symptoms which included: Deep Bite, Anterior Open Bite, and Posterior Open Bite. This is part 3, we will be discussing the last of the TMD symptoms: Anterior Crossbite, Posterior Crossbite, and Functional Shift of the Mandible. Prelude: When orthodontics and other dentistry is delivered elegantly there is a fusion between aesthetics, tooth function and TMJ health. assessment AND Part 3: Why Orthodontics is the TREATMENT: Best Treatment for Most TMJ Patients By Ralph Nicassio, DDS and Maria Zavala, RDA Fig. 2 I Besides TMD, patients with crossbite often express other stomatognathic problems including but not limited to: í Para-functional tooth wear, abrasions, fractions, non-hygiene related tissue recession í Strained Swallowing musculature í Impaired speaking í Functional shift of the mandible í Limitations on esthetics í Canted occlusal plane í Facial asymmetry CRossbITE ANTERIoR CRossbITE Anterior crossbite can be corrected in 5 ways: 3 TMD is highly associated with crossbite which can take the following forms: 1,2 í Anterior crossbite í Unilateral posterior crossbite í Bilateral posterior crossbite í Hidden posterior crossbite that may not be obvi-ously present but demonstrates once proper phys-iological position of the mandible is established. ᕡ The first and unfortunately most common method for correction of anterior crossbite is making some appliance that results in tipping of the anterior teeth forward. Virtually all remove-able appliances work by tipping the clinical crowns. (Fig. 1) ᕢ The 2nd method for correction of anterior cross-bite is bodily advancement of the maxilla with Reverse Headgear (RHG, also known as protraction head gear or a facemask). This is most ideally done 18 Winter 2018 JAOS
Journal of the American Orthodontic Society Winter 2018: Page 18