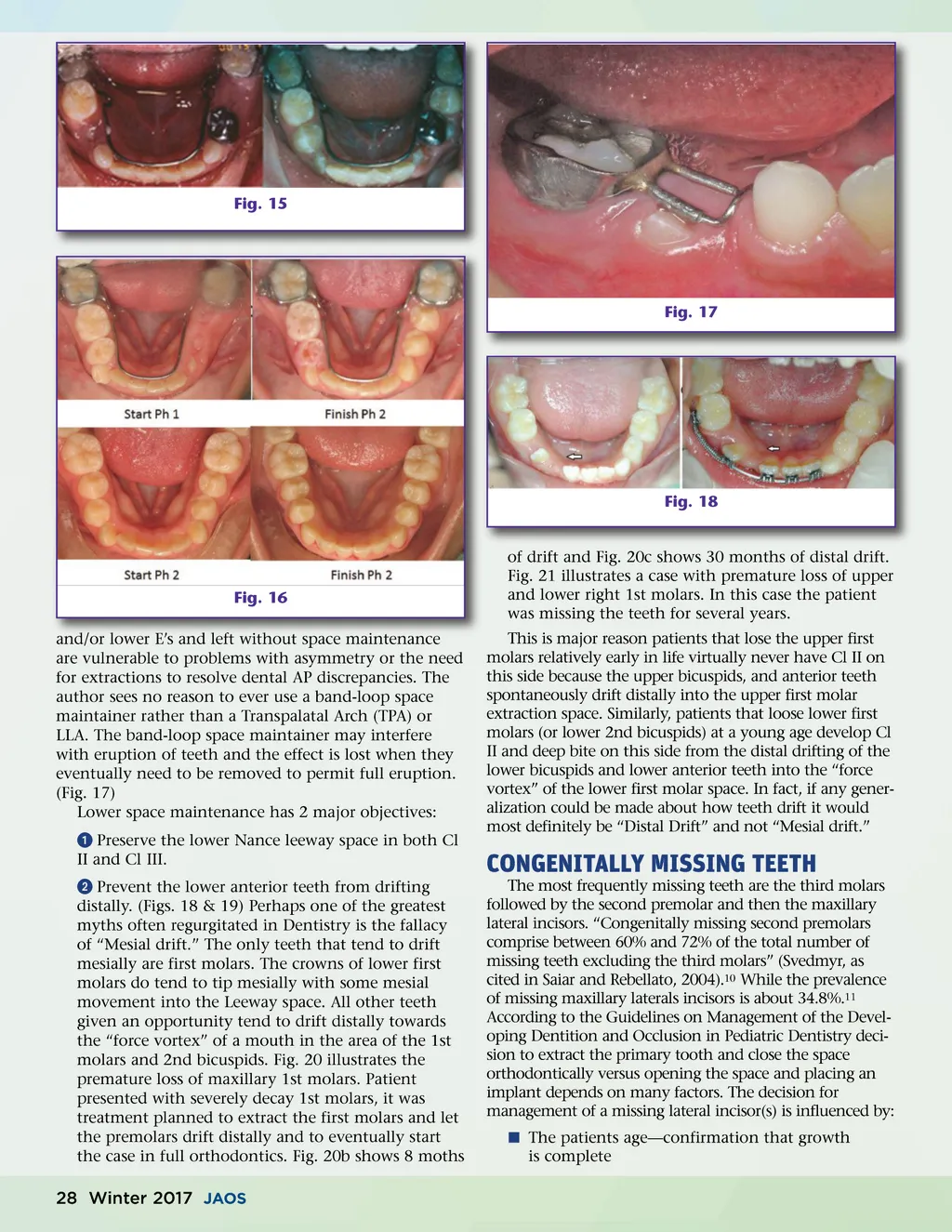
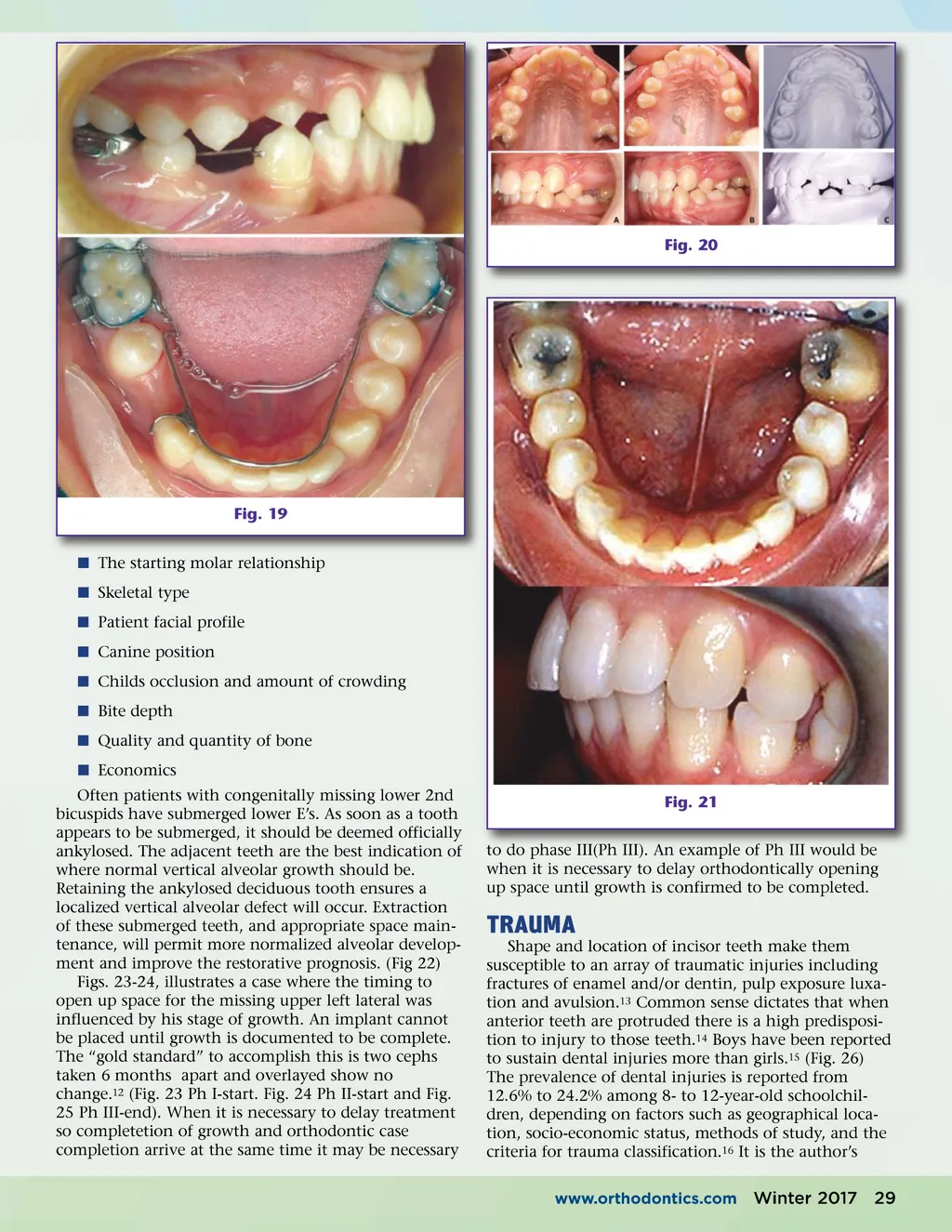
Fig. 20 Fig. 19 í The starting molar relationship í Skeletal type í Patient facial profile í Canine position í Childs occlusion and amount of crowding í Bite depth í Quality and quantity of bone í Economics Often patients with congenitally missing lower 2nd bicuspids have submerged lower E’s. As soon as a tooth appears to be submerged, it should be deemed officially ankylosed. The adjacent teeth are the best indication of where normal vertical alveolar growth should be. Retaining the ankylosed deciduous tooth ensures a localized vertical alveolar defect will occur. Extraction of these submerged teeth, and appropriate space main-tenance, will permit more normalized alveolar develop-ment and improve the restorative prognosis. (Fig 22) Figs. 23-24, illustrates a case where the timing to open up space for the missing upper left lateral was influenced by his stage of growth. An implant cannot be placed until growth is documented to be complete. The “gold standard” to accomplish this is two cephs taken 6 months apart and overlayed show no change. 12 (Fig. 23 Ph I-start. Fig. 24 Ph II-start and Fig. 25 Ph III-end). When it is necessary to delay treatment so completetion of growth and orthodontic case completion arrive at the same time it may be necessary Fig. 21 to do phase III(Ph III). An example of Ph III would be when it is necessary to delay orthodontically opening up space until growth is confirmed to be completed. TRAUMA Shape and location of incisor teeth make them susceptible to an array of traumatic injuries including fractures of enamel and/or dentin, pulp exposure luxa-tion and avulsion. 13 Common sense dictates that when anterior teeth are protruded there is a high predisposi-tion to injury to those teeth. 14 Boys have been reported to sustain dental injuries more than girls. 15 (Fig. 26) The prevalence of dental injuries is reported from 12.6% to 24.2% among 8-to 12-year-old schoolchil-dren, depending on factors such as geographical loca-tion, socio-economic status, methods of study, and the criteria for trauma classification. 16 It is the author’s www.orthodontics.com Winter 2017 29
Journal of the American Orthodontic Society Winter 2017: Page 29