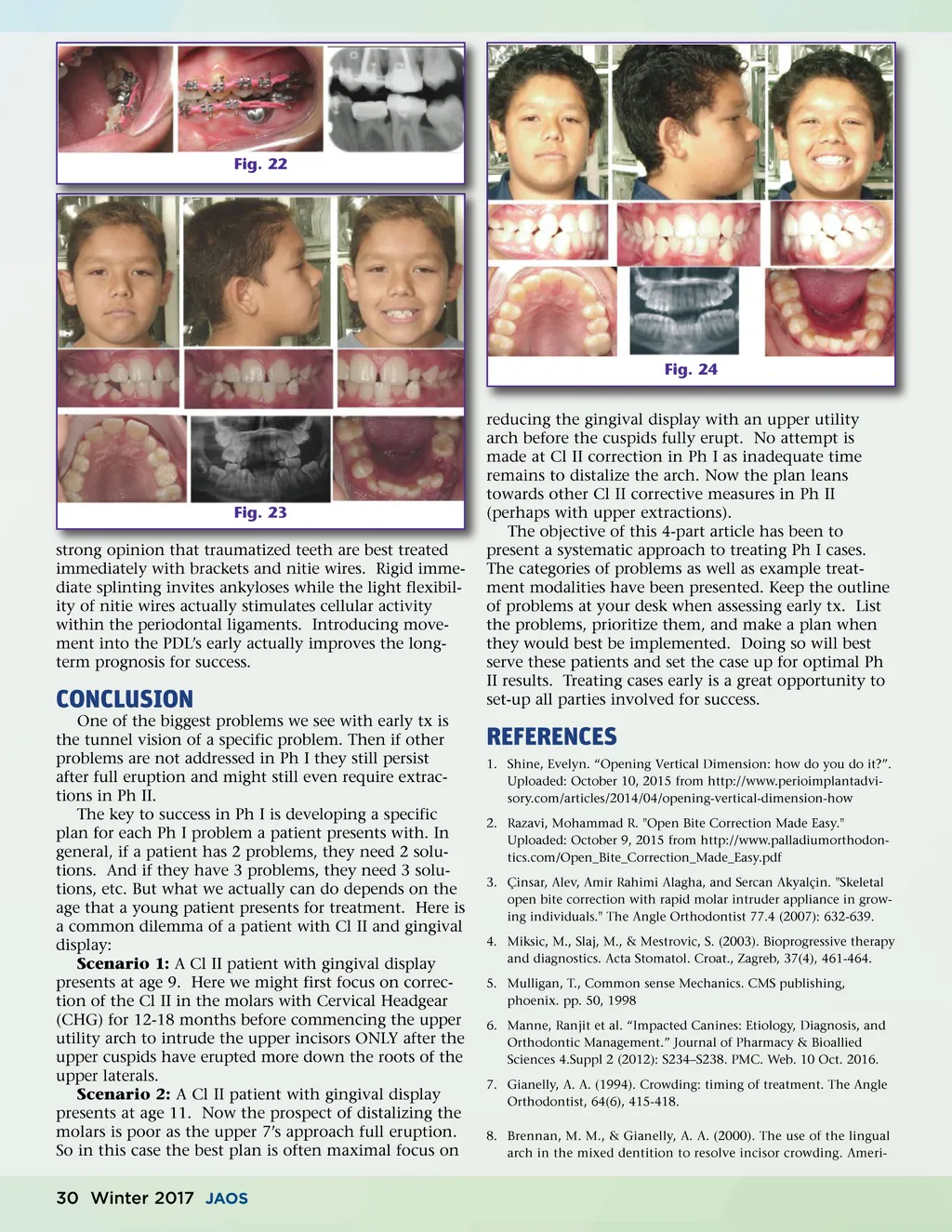
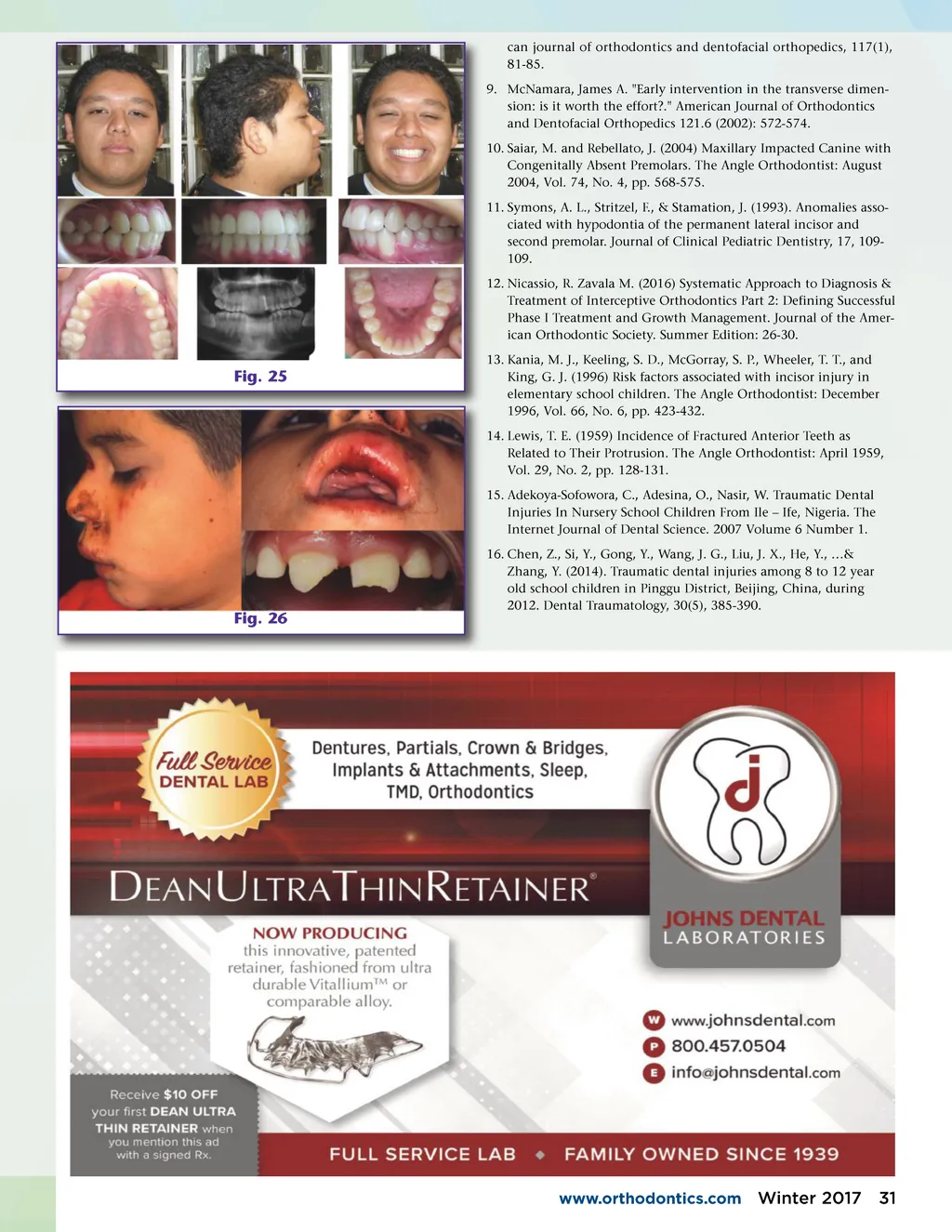
Fig. 22 Fig. 24 reducing the gingival display with an upper utility arch before the cuspids fully erupt. No attempt is made at Cl II correction in Ph I as inadequate time remains to distalize the arch. Now the plan leans towards other Cl II corrective measures in Ph II (perhaps with upper extractions). The objective of this 4-part article has been to present a systematic approach to treating Ph I cases. The categories of problems as well as example treat-ment modalities have been presented. Keep the outline of problems at your desk when assessing early tx. List the problems, prioritize them, and make a plan when they would best be implemented. Doing so will best serve these patients and set the case up for optimal Ph II results. Treating cases early is a great opportunity to set-up all parties involved for success. Fig. 23 strong opinion that traumatized teeth are best treated immediately with brackets and nitie wires. Rigid imme-diate splinting invites ankyloses while the light flexibil-ity of nitie wires actually stimulates cellular activity within the periodontal ligaments. Introducing move-ment into the PDL’s early actually improves the long-term prognosis for success. CONCLUSION One of the biggest problems we see with early tx is the tunnel vision of a specific problem. Then if other problems are not addressed in Ph I they still persist after full eruption and might still even require extrac-tions in Ph II. The key to success in Ph I is developing a specific plan for each Ph I problem a patient presents with. In general, if a patient has 2 problems, they need 2 solu-tions. And if they have 3 problems, they need 3 solu-tions, etc. But what we actually can do depends on the age that a young patient presents for treatment. Here is a common dilemma of a patient with Cl II and gingival display: Scenario 1: A Cl II patient with gingival display presents at age 9. Here we might first focus on correc-tion of the Cl II in the molars with Cervical Headgear (CHG) for 12-18 months before commencing the upper utility arch to intrude the upper incisors ONLY after the upper cuspids have erupted more down the roots of the upper laterals. Scenario 2: A Cl II patient with gingival display presents at age 11. Now the prospect of distalizing the molars is poor as the upper 7’s approach full eruption. So in this case the best plan is often maximal focus on REFERENCES 1. Shine, Evelyn. “Opening Vertical Dimension: how do you do it?”. Uploaded: October 10, 2015 from http://www.perioimplantadvi-sory.com/articles/2014/04/opening-vertical-dimension-how 2. Razavi, Mohammad R. "Open Bite Correction Made Easy." Uploaded: October 9, 2015 from http://www.palladiumorthodon-tics.com/Open_Bite_Correction_Made_Easy.pdf 3. Çinsar, Alev, Amir Rahimi Alagha, and Sercan Akyalçin. "Skeletal open bite correction with rapid molar intruder appliance in grow-ing individuals." The Angle Orthodontist 77.4 (2007): 632-639. 4. Miksic, M., Slaj, M., & Mestrovic, S. (2003). Bioprogressive therapy and diagnostics. Acta Stomatol. Croat., Zagreb, 37(4), 461-464. 5. Mulligan, T., Common sense Mechanics. CMS publishing, phoenix. pp. 50, 1998 6. Manne, Ranjit et al. “Impacted Canines: Etiology, Diagnosis, and Orthodontic Management.” Journal of Pharmacy & Bioallied Sciences 4.Suppl 2 (2012): S234–S238. PMC. Web. 10 Oct. 2016. 7. Gianelly, A. A. (1994). Crowding: timing of treatment. The Angle Orthodontist, 64(6), 415-418. 8. Brennan, M. M., & Gianelly, A. A. (2000). The use of the lingual arch in the mixed dentition to resolve incisor crowding. Ameri-30 Winter 2017 JAOS
Journal of the American Orthodontic Society Winter 2017: Page 30