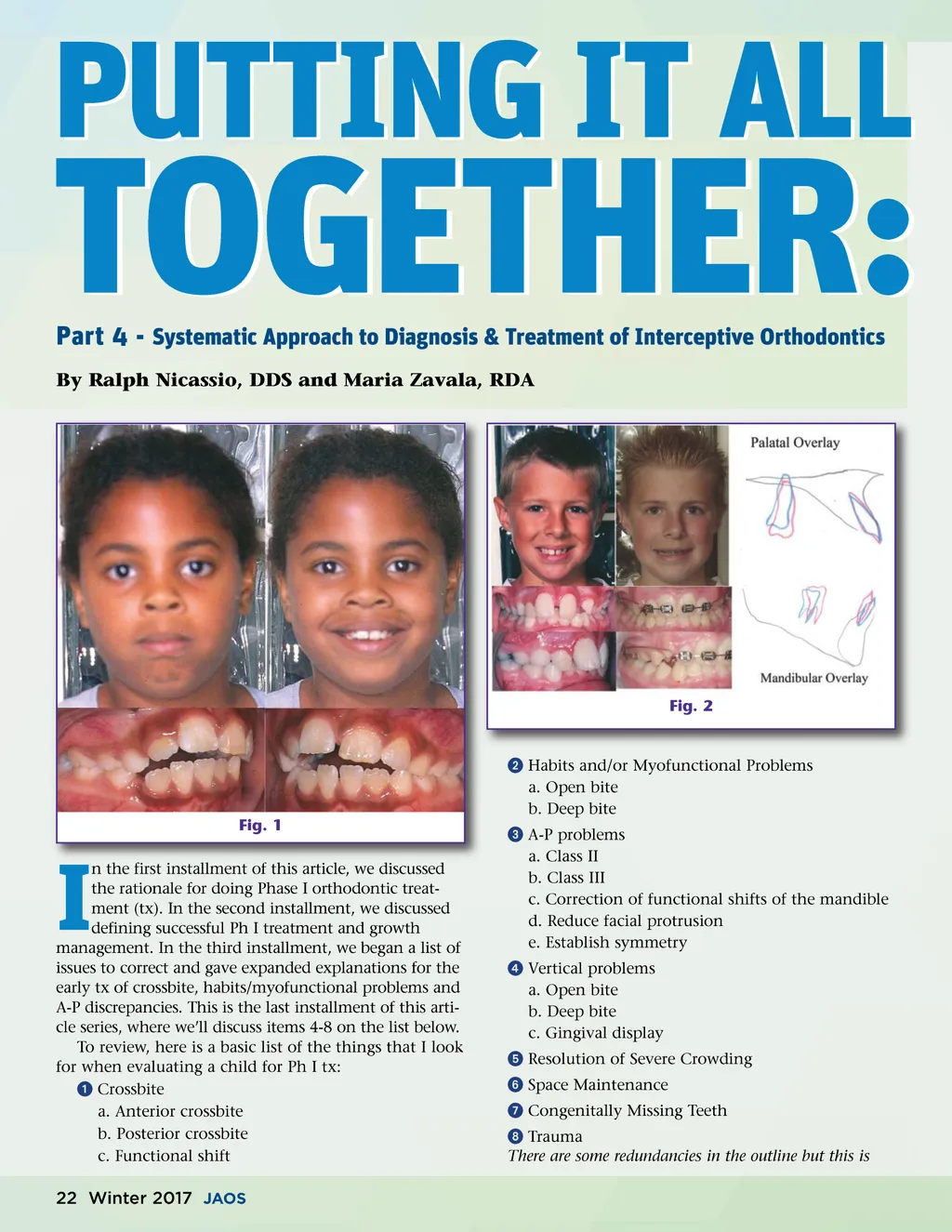
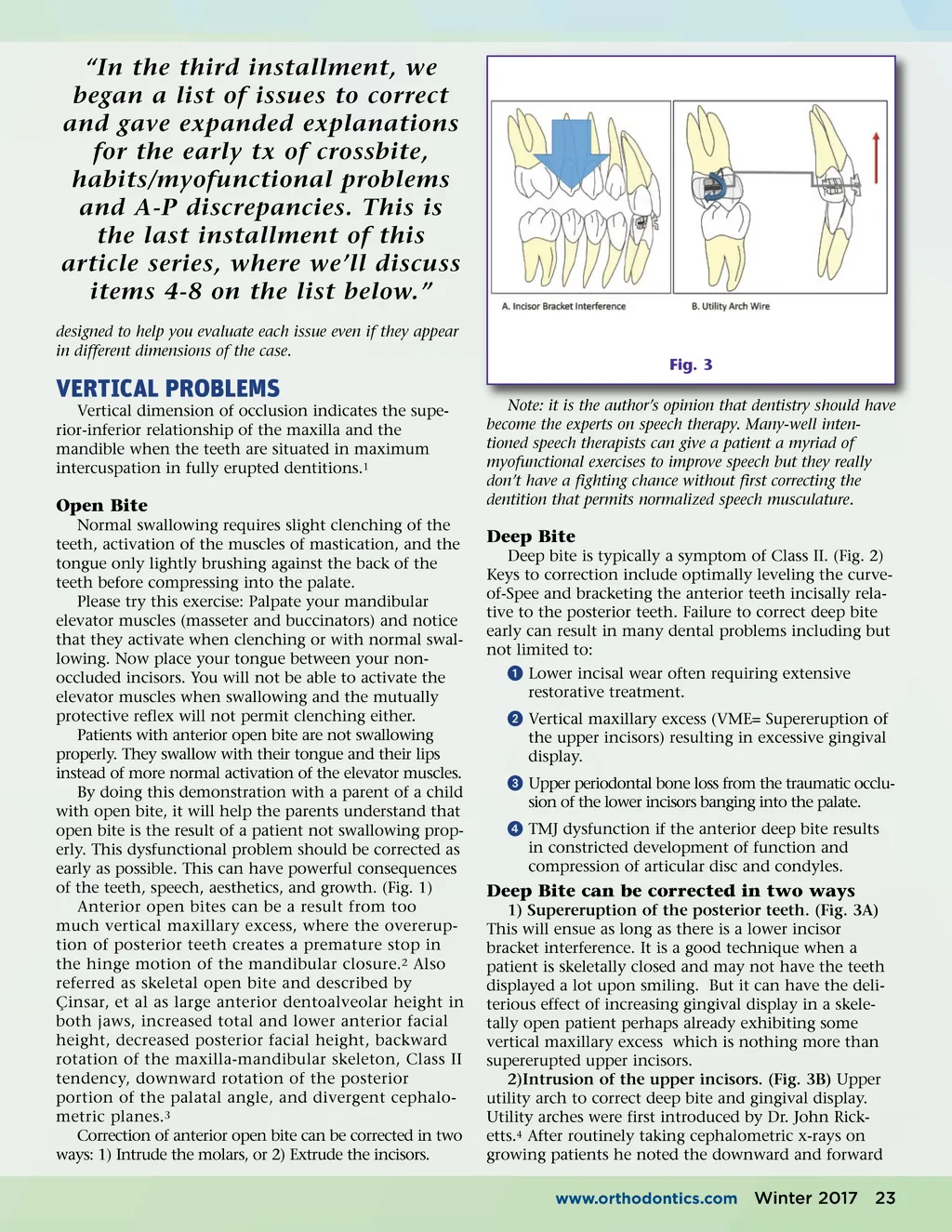
“In the third installment, we began a list of issues to correct and gave expanded explanations for the early tx of crossbite, habits/myofunctional problems and A-P discrepancies. This is the last installment of this article series, where we’ll discuss items 4-8 on the list below.” designed to help you evaluate each issue even if they appear in different dimensions of the case. Fig. 3 Note: it is the author’s opinion that dentistry should have become the experts on speech therapy. Many-well inten-tioned speech therapists can give a patient a myriad of myofunctional exercises to improve speech but they really don’t have a fighting chance without first correcting the dentition that permits normalized speech musculature. VERTICAL PROBLEMS Vertical dimension of occlusion indicates the supe-rior-inferior relationship of the maxilla and the mandible when the teeth are situated in maximum intercuspation in fully erupted dentitions. 1 Open Bite Normal swallowing requires slight clenching of the teeth, activation of the muscles of mastication, and the tongue only lightly brushing against the back of the teeth before compressing into the palate. Please try this exercise: Palpate your mandibular elevator muscles (masseter and buccinators) and notice that they activate when clenching or with normal swal-lowing. Now place your tongue between your non-occluded incisors. You will not be able to activate the elevator muscles when swallowing and the mutually protective reflex will not permit clenching either. Patients with anterior open bite are not swallowing properly. They swallow with their tongue and their lips instead of more normal activation of the elevator muscles. By doing this demonstration with a parent of a child with open bite, it will help the parents understand that open bite is the result of a patient not swallowing prop-erly. This dysfunctional problem should be corrected as early as possible. This can have powerful consequences of the teeth, speech, aesthetics, and growth. (Fig. 1) Anterior open bites can be a result from too much vertical maxillary excess, where the overerup-tion of posterior teeth creates a premature stop in the hinge motion of the mandibular closure. 2 Also referred as skeletal open bite and described by Çinsar, et al as large anterior dentoalveolar height in both jaws, increased total and lower anterior facial height, decreased posterior facial height, backward rotation of the maxilla-mandibular skeleton, Class II tendency, downward rotation of the posterior portion of the palatal angle, and divergent cephalo-metric planes. 3 Correction of anterior open bite can be corrected in two ways: 1) Intrude the molars, or 2) Extrude the incisors. Deep Bite Deep bite is typically a symptom of Class II. (Fig. 2) Keys to correction include optimally leveling the curve-of-Spee and bracketing the anterior teeth incisally rela-tive to the posterior teeth. Failure to correct deep bite early can result in many dental problems including but not limited to: ᕡ Lower incisal wear often requiring extensive restorative treatment. ᕢ Vertical maxillary excess (VME= Supereruption of the upper incisors) resulting in excessive gingival display. ᕣ Upper periodontal bone loss from the traumatic occlu-sion of the lower incisors banging into the palate. ᕤ TMJ dysfunction if the anterior deep bite results in constricted development of function and compression of articular disc and condyles. Deep Bite can be corrected in two ways 1) Supereruption of the posterior teeth. (Fig. 3A) This will ensue as long as there is a lower incisor bracket interference. It is a good technique when a patient is skeletally closed and may not have the teeth displayed a lot upon smiling. But it can have the deli-terious effect of increasing gingival display in a skele-tally open patient perhaps already exhibiting some vertical maxillary excess which is nothing more than supererupted upper incisors. 2)Intrusion of the upper incisors. (Fig. 3B) Upper utility arch to correct deep bite and gingival display. Utility arches were first introduced by Dr. John Rick-etts. 4 After routinely taking cephalometric x-rays on growing patients he noted the downward and forward www.orthodontics.com Winter 2017 23
Journal of the American Orthodontic Society Winter 2017: Page 23