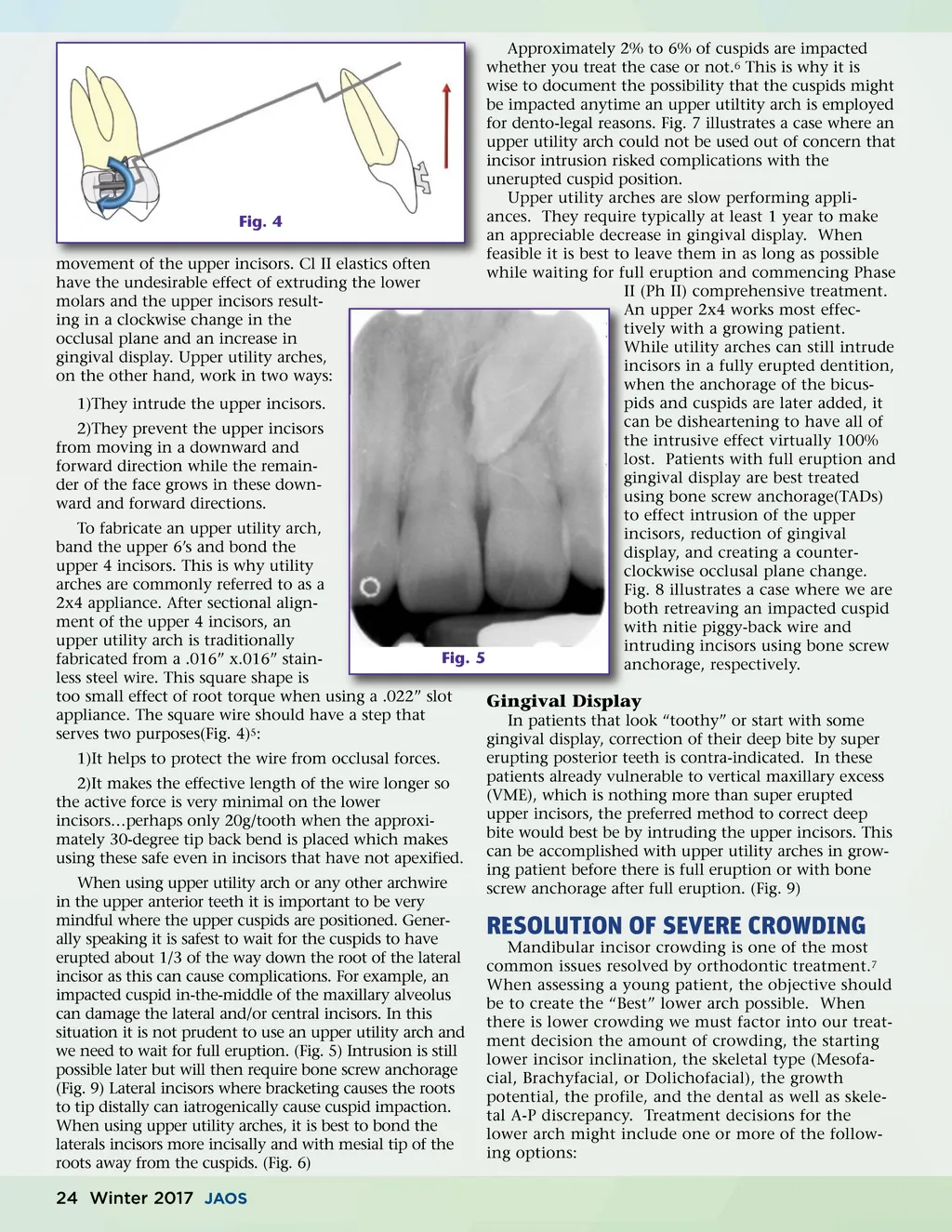
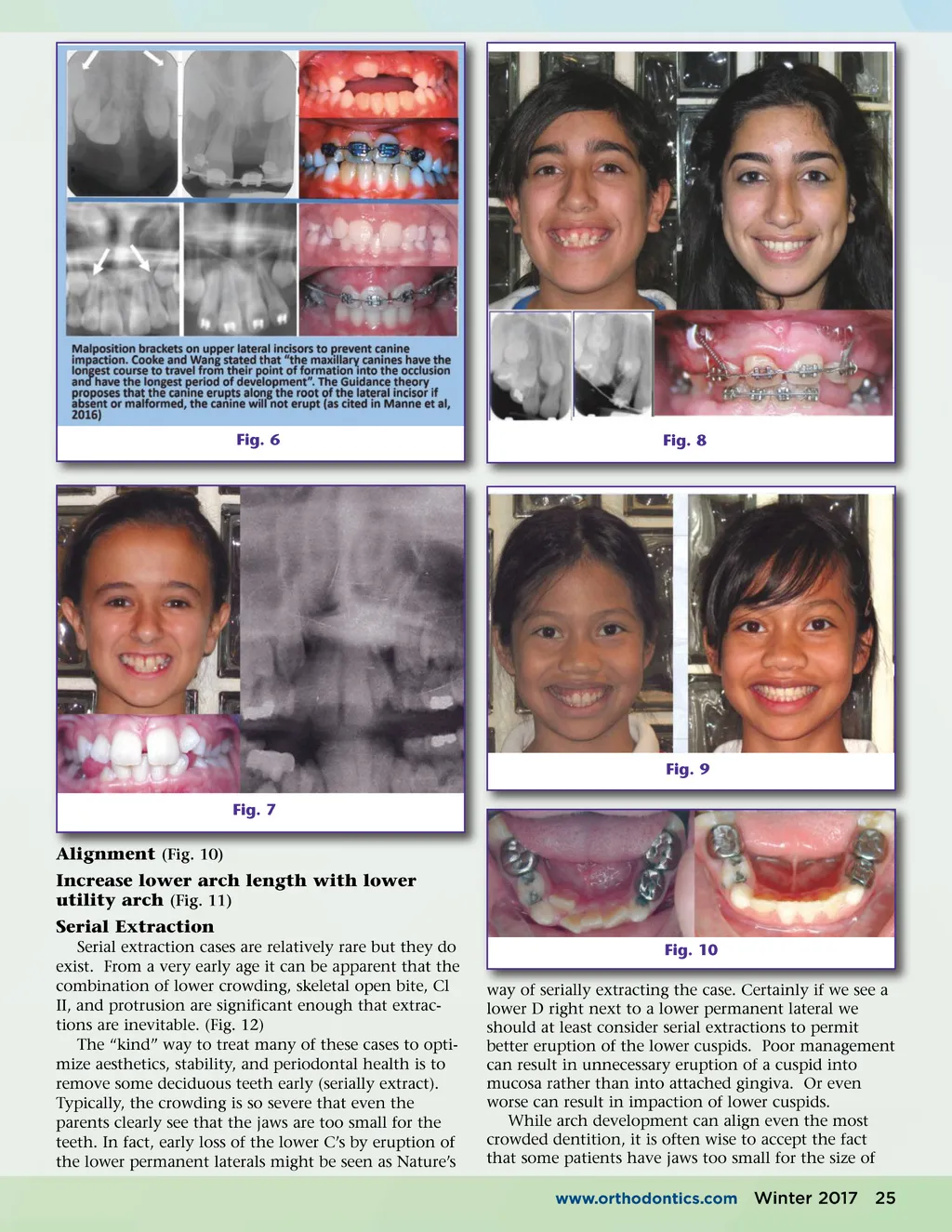
Approximately 2% to 6% of cuspids are impacted whether you treat the case or not. 6 This is why it is wise to document the possibility that the cuspids might be impacted anytime an upper utiltity arch is employed for dento-legal reasons. Fig. 7 illustrates a case where an upper utility arch could not be used out of concern that incisor intrusion risked complications with the unerupted cuspid position. Upper utility arches are slow performing appli-ances. They require typically at least 1 year to make Fig. 4 an appreciable decrease in gingival display. When feasible it is best to leave them in as long as possible movement of the upper incisors. Cl II elastics often while waiting for full eruption and commencing Phase have the undesirable effect of extruding the lower II (Ph II) comprehensive treatment. molars and the upper incisors result-An upper 2x4 works most effec-ing in a clockwise change in the tively with a growing patient. occlusal plane and an increase in While utility arches can still intrude gingival display. Upper utility arches, incisors in a fully erupted dentition, on the other hand, work in two ways: when the anchorage of the bicus-pids and cuspids are later added, it 1)They intrude the upper incisors. can be disheartening to have all of 2)They prevent the upper incisors the intrusive effect virtually 100% from moving in a downward and lost. Patients with full eruption and forward direction while the remain-gingival display are best treated der of the face grows in these down-using bone screw anchorage(TADs) ward and forward directions. to effect intrusion of the upper To fabricate an upper utility arch, incisors, reduction of gingival band the upper 6’s and bond the display, and creating a counter-upper 4 incisors. This is why utility clockwise occlusal plane change. arches are commonly referred to as a Fig. 8 illustrates a case where we are 2x4 appliance. After sectional align-both retreaving an impacted cuspid ment of the upper 4 incisors, an with nitie piggy-back wire and upper utility arch is traditionally intruding incisors using bone screw Fig. 5 fabricated from a .016” x.016” stain-anchorage, respectively. less steel wire. This square shape is too small effect of root torque when using a .022” slot Gingival Display appliance. The square wire should have a step that In patients that look “toothy” or start with some serves two purposes(Fig. 4) 5 : gingival display, correction of their deep bite by super 1)It helps to protect the wire from occlusal forces. 2)It makes the effective length of the wire longer so the active force is very minimal on the lower incisors…perhaps only 20g/tooth when the approxi-mately 30-degree tip back bend is placed which makes using these safe even in incisors that have not apexified. When using upper utility arch or any other archwire in the upper anterior teeth it is important to be very mindful where the upper cuspids are positioned. Gener-ally speaking it is safest to wait for the cuspids to have erupted about 1/3 of the way down the root of the lateral incisor as this can cause complications. For example, an impacted cuspid in-the-middle of the maxillary alveolus can damage the lateral and/or central incisors. In this situation it is not prudent to use an upper utility arch and we need to wait for full eruption. (Fig. 5) Intrusion is still possible later but will then require bone screw anchorage (Fig. 9) Lateral incisors where bracketing causes the roots to tip distally can iatrogenically cause cuspid impaction. When using upper utility arches, it is best to bond the laterals incisors more incisally and with mesial tip of the roots away from the cuspids. (Fig. 6) erupting posterior teeth is contra-indicated. In these patients already vulnerable to vertical maxillary excess (VME), which is nothing more than super erupted upper incisors, the preferred method to correct deep bite would best be by intruding the upper incisors. This can be accomplished with upper utility arches in grow-ing patient before there is full eruption or with bone screw anchorage after full eruption. (Fig. 9) RESOLUTION OF SEVERE CROWDING Mandibular incisor crowding is one of the most common issues resolved by orthodontic treatment. 7 When assessing a young patient, the objective should be to create the “Best” lower arch possible. When there is lower crowding we must factor into our treat-ment decision the amount of crowding, the starting lower incisor inclination, the skeletal type (Mesofa-cial, Brachyfacial, or Dolichofacial), the growth potential, the profile, and the dental as well as skele-tal A-P discrepancy. Treatment decisions for the lower arch might include one or more of the follow-ing options: 24 Winter 2017 JAOS
Journal of the American Orthodontic Society Winter 2017: Page 24