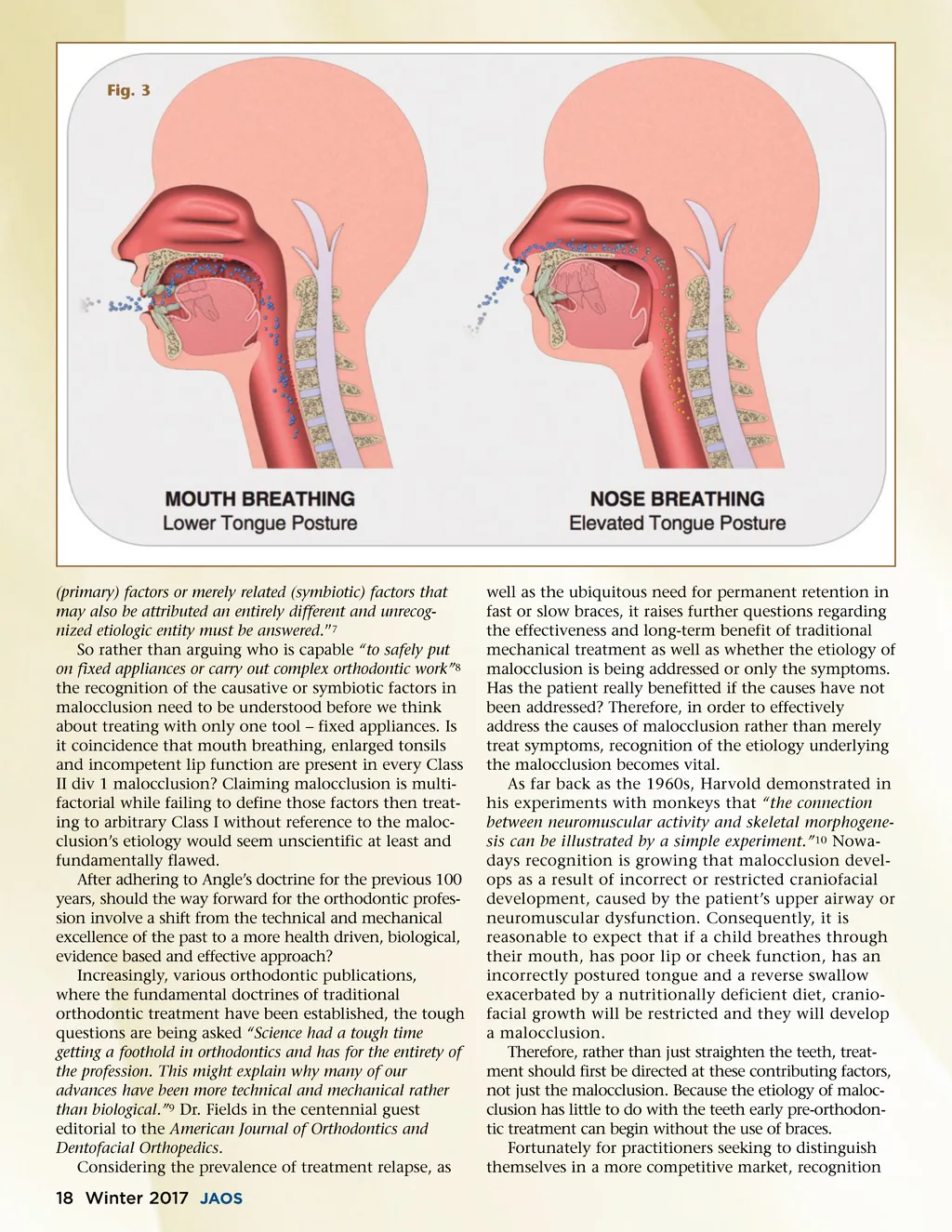
Fig. 3 (primary) factors or merely related (symbiotic) factors that may also be attributed an entirely different and unrecog-nized etiologic entity must be answered. ” 7 So rather than arguing who is capable “to safely put on fixed appliances or carry out complex orthodontic work” 8 the recognition of the causative or symbiotic factors in malocclusion need to be understood before we think about treating with only one tool – fixed appliances. Is it coincidence that mouth breathing, enlarged tonsils and incompetent lip function are present in every Class II div 1 malocclusion? Claiming malocclusion is multi-factorial while failing to define those factors then treat-ing to arbitrary Class I without reference to the maloc-clusion’s etiology would seem unscientific at least and fundamentally flawed. After adhering to Angle’s doctrine for the previous 100 years, should the way forward for the orthodontic profes-sion involve a shift from the technical and mechanical excellence of the past to a more health driven, biological, evidence based and effective approach? Increasingly, various orthodontic publications, where the fundamental doctrines of traditional orthodontic treatment have been established, the tough questions are being asked “Science had a tough time getting a foothold in orthodontics and has for the entirety of the profession. This might explain why many of our advances have been more technical and mechanical rather than biological.” 9 Dr. Fields in the centennial guest editorial to the American Journal of Orthodontics and Dentofacial Orthopedics . Considering the prevalence of treatment relapse, as well as the ubiquitous need for permanent retention in fast or slow braces, it raises further questions regarding the effectiveness and long-term benefit of traditional mechanical treatment as well as whether the etiology of malocclusion is being addressed or only the symptoms. Has the patient really benefitted if the causes have not been addressed? Therefore, in order to effectively address the causes of malocclusion rather than merely treat symptoms, recognition of the etiology underlying the malocclusion becomes vital. As far back as the 1960s, Harvold demonstrated in his experiments with monkeys that “the connection between neuromuscular activity and skeletal morphogene-sis can be illustrated by a simple experiment.” 10 Nowa-days recognition is growing that malocclusion devel-ops as a result of incorrect or restricted craniofacial development, caused by the patient’s upper airway or neuromuscular dysfunction. Consequently, it is reasonable to expect that if a child breathes through their mouth, has poor lip or cheek function, has an incorrectly postured tongue and a reverse swallow exacerbated by a nutritionally deficient diet, cranio-facial growth will be restricted and they will develop a malocclusion. Therefore, rather than just straighten the teeth, treat-ment should first be directed at these contributing factors, not just the malocclusion. Because the etiology of maloc-clusion has little to do with the teeth early pre-orthodon-tic treatment can begin without the use of braces. Fortunately for practitioners seeking to distinguish themselves in a more competitive market, recognition 18 Winter 2017 JAOS
Journal of the American Orthodontic Society Winter 2017: Page 18