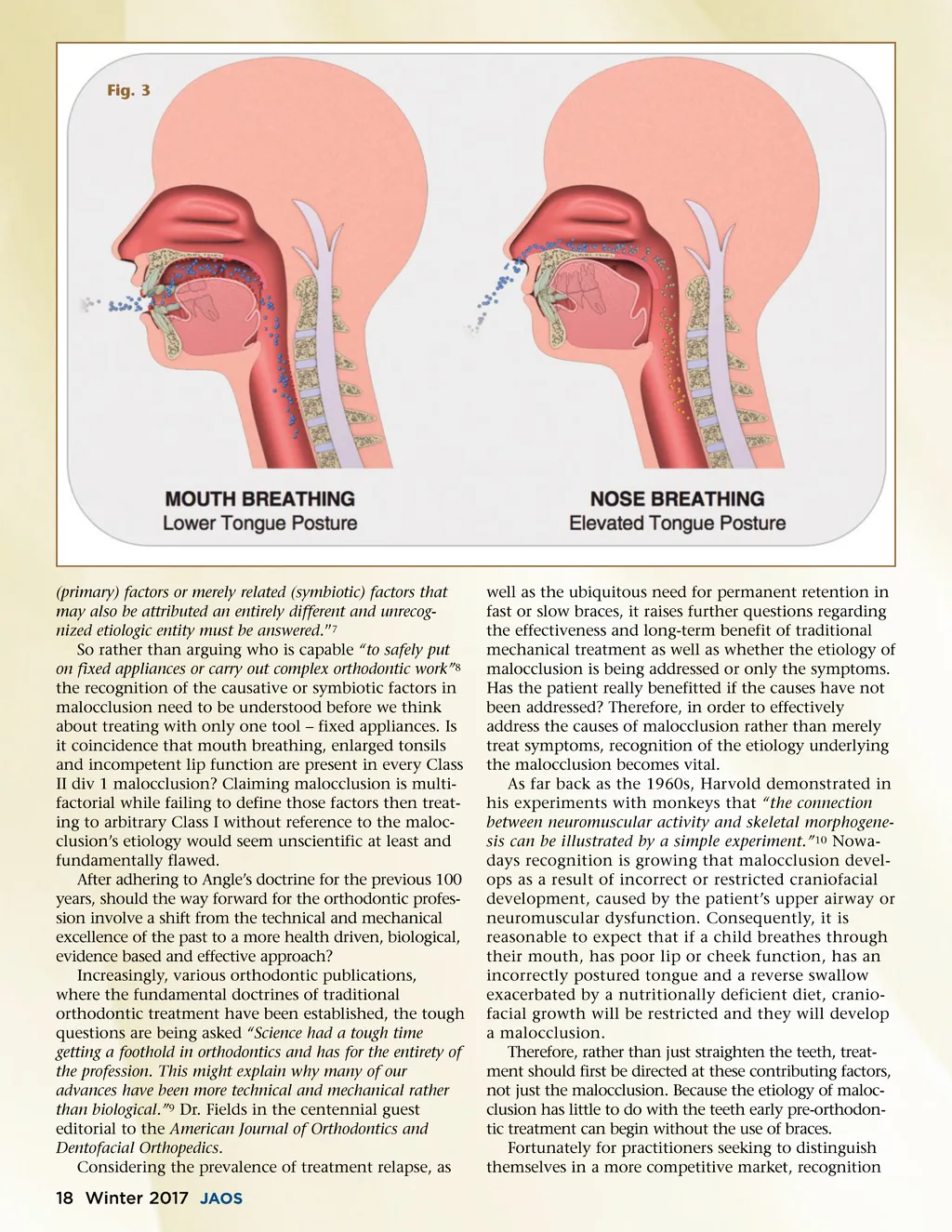
of the effect upper airway and neuromuscular dysfunc-tion has on craniofacial growth and therefore, maloc-clusion, has prompted a change in ideology. As a result, focus has shifted from the technical and mechanical excellence of the past towards more health driven, biological, evidence based and effective approaches to correcting or preferably preventing malocclusion alto-gether. Orthodontic journals are now publishing more on the importance of airways in the overall health and well being of a child and the impact of orthodontics on airway and a lifetime of better health. However, it was really there all the time and we missed Graber’s, Harvold’s and Ricketts’ biological approach. The author penned the title ‘myofunctional orthodontics’ 30 years ago. It could also be called etio-logic orthodontics. The core tenets of myofunctional orthodontics are aimed towards addressing the etiologi-cal causes of malocclusion. Rather than just straighten-ing teeth into an arbitrary Class I and then retaining forever, myofunctional orthodontic practitioners target the upper airway and neuromuscular dysfunction, which inhibits craniofacial development. Furthermore, by focusing on the etiology of the malocclusion and promoting correct growth in the primary or early mixed dentition, teeth are often provided with the space required to move into the correct alignment naturally, “and often the teeth will come in straight even before you get to the braces.” 11 According to New Jersey Orthodontist Dr. Barry Raphael, “Just as the future of medicine has to be looking at root cause, the future of orthodontics is also going to be looking at root cause.” 12 The rectification of the etiological factors restricting development can not only correct malocclusion, with myofunctional orthodontics it is possible to begin treat-ment while the patient is young enough to satisfy the increasing demand from parents for early orthodontic intervention. Because “ the optimal timing for myofunc-tional intervention is a period of active growth and develop-ment with high adaptive capacity” 13 upper airway and neuromuscular dysfunction can be corrected before it reaches a severity “which would require considerable efforts to correct later in life.” 14 Because during “the last 100 years, no one has been able to produce scientific evidence to corroborate Bonwill and Angle’s original hypothesis” 15 and the only advances in orthodontic practice have been mechani-cal; myofunctional orthodontics represents a logical step forward. According to the American Journal of Orthodontics and Dentofacial Orthopedics “Research presented in our Journal in the next century may shed new light that will help us better identify the problem and aid the specialty in developing more effective evidence-based treatment” 16 which indicates orthodontics is already moving in this direction. When considering the challenges, the orthodontic profession is faced with today, this change of direction cannot come soon enough. Today specialists no longer have a monopoly on orthodontic care. Technology has enabled access for more patients who are predomi-nantly treated using century old mechanical doctrines Myofunctional orthodontics focuses on treating the etiology of malocclusion to achieve lifelong natural health outcomes by establishing nasal breathing as a primary goal. by either orthodontic specialists or by pediatric and general dentist. Compounding this is the oversupply of new dental professionals and corporatization of the dental industry where orthodontic care has been rele-gated to a mere commodity where the dollar value can become more important than a patient’s health and well-being. However, myofunctional orthodontics requires a new paradigm in learning for the specialty of orthodon-tics, which tends to be behind on acquiring the diag-nostic skills to safely “carry out complex (myofunctional) orthodontic work” 17 in growing children in the future. The time has come to learn new skills. For some orthodontic practitioners, reliant on the traditional orthodontic standard of care, profitability of the past is diminishing, and the future is far from assured. However, for forward-thinking practitioners it has presented the opportunity to play an active role in shaping the profession’s future by looking towards new treatment systems, which are evidence based and health driven rather than focused on just mechanically straightening the teeth into an arbitrary Class I. In fact, when considering “the history of how orthodontic educa-tion evolved, it is easy to see how the specialty could grow, flow, and turn with ideas and views that were not science-based and were provided by a selected few persons.” 18 Myofunctional orthodontics, which is focused on treating the etiology of malocclusion to achieve lifelong natural health outcomes by establishing nasal breath-ing as a primary goal, provides a means for today’s practitioners to distinguish themselves from the crowd. Additionally, there are new opportunities emerging that offer the prospect for forward thinking orthodontic professionals to work with members of the medical profession and offer solutions for the health issues related to Sleep Disordered Breathing (SDB). (Fig.3) “Since the beginning of our specialty, our understanding of the link between function and facial growth and develop-ment has progressively improved. Today, we know that chil-dren with sleep-related breathing problems will often develop distinctive facial characteristics.” 19 Furthermore, pediatric SDB has been recognized as causing widespread health, developmental and behav-ioral problems, including difficulty concentrating at www.orthodontics.com Winter 2017 19
Journal of the American Orthodontic Society Winter 2017: Page 19