By Edward Burgess Jones, DDS, FAGD, FPFA, DABFE, DABFM, DABFD, FRSH, FADI n dentistry the metal nickel is a cause of concern for both orthodontists and general dentists. It is commonly used in the field of dentistry and is the most common cause of dermatitis or allergic response. 1,2,3 Nickel has sometimes been i ndicated as a biological and histological sensitizer that can cause short and long term reactions (Type IV immune response). However, it seldom results in discontinu-ance of treatment due to any severe adverse reactions to the patient. 4,5,6,7 We report on a patient undergoing routine orthodontic treatment. Within an hour follow-ing the placement of the orthodontic appliances (brackets) and wires the patient was rushed to the emergency room because of difficulty in breathing and the appearance of a significant generalized body rash. A diagnosis of extreme reaction to the metal nickel was made at the hospital. This article discusses the clinical and diagnostic aspects of orthodontic appliances containing the metal nickel and the histopathologic aspects of an allergic patient undergoing orthodontic treatment. It emphasizes the accuracy of a thorough patient health history and the completeness of the family history to allergies. Patients undergoing orthodontic care rarely experi-ence allergies to the components within the orthodon-I tic treatment appliances. Although there is mounting evidence that metal braces may be a contributor to localized gingival erythemia and hypertrophy of gingi-val tissue. 8,9,10 Most often better oral hygiene seems to ameliorate the condition. When any metal is used in fixed and removable orthodontic appliances the metal of choice is stainless steel and a component is metal nickel, atomic number 28. The presence of this metal has demonstrated on rare occasions to be a possible biological and histologic sensitizer to human tissues. 11,12 Although allergies that cause short term and long term reactions are rare they can still occur. 13,14,15 This is one such case. The health history is probably the most important part of assessing the criteria for patient care. CASE PRESENTATION The patient a 15 year old Caucasian male student 5’ 6” tall and a weight of 126 pounds presented for routine orthodontic treatment. His initial diagnosis and treatment plan included the management of a class I dental occlusion with slight maxillary mid-face retrusion and insufficient dental arch form. The health history provided by the patient and family was negative to any types of allergies or any other health 36 Winter 2016 JAOS
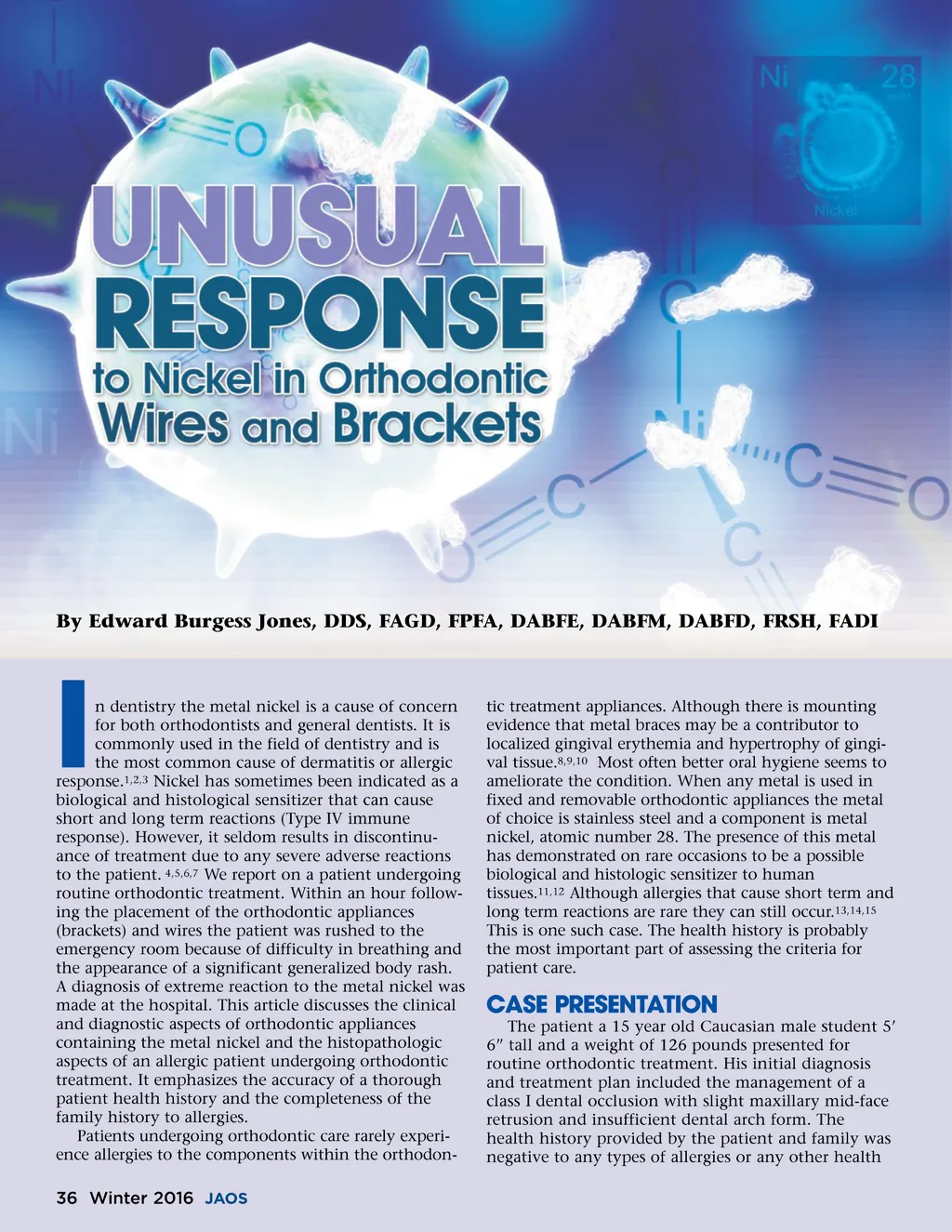
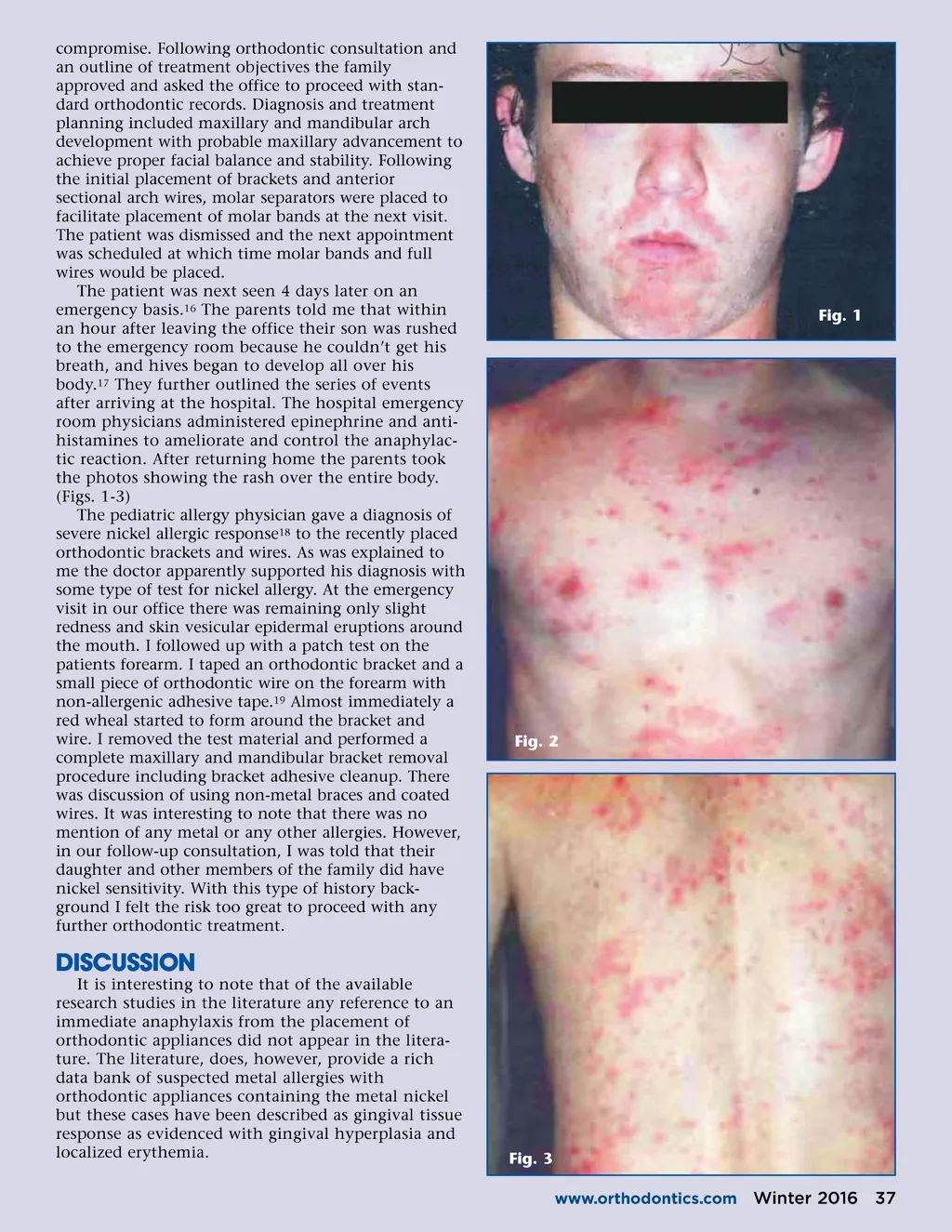
Journal of the American Orthodontic Society Winter 2016: Page 36