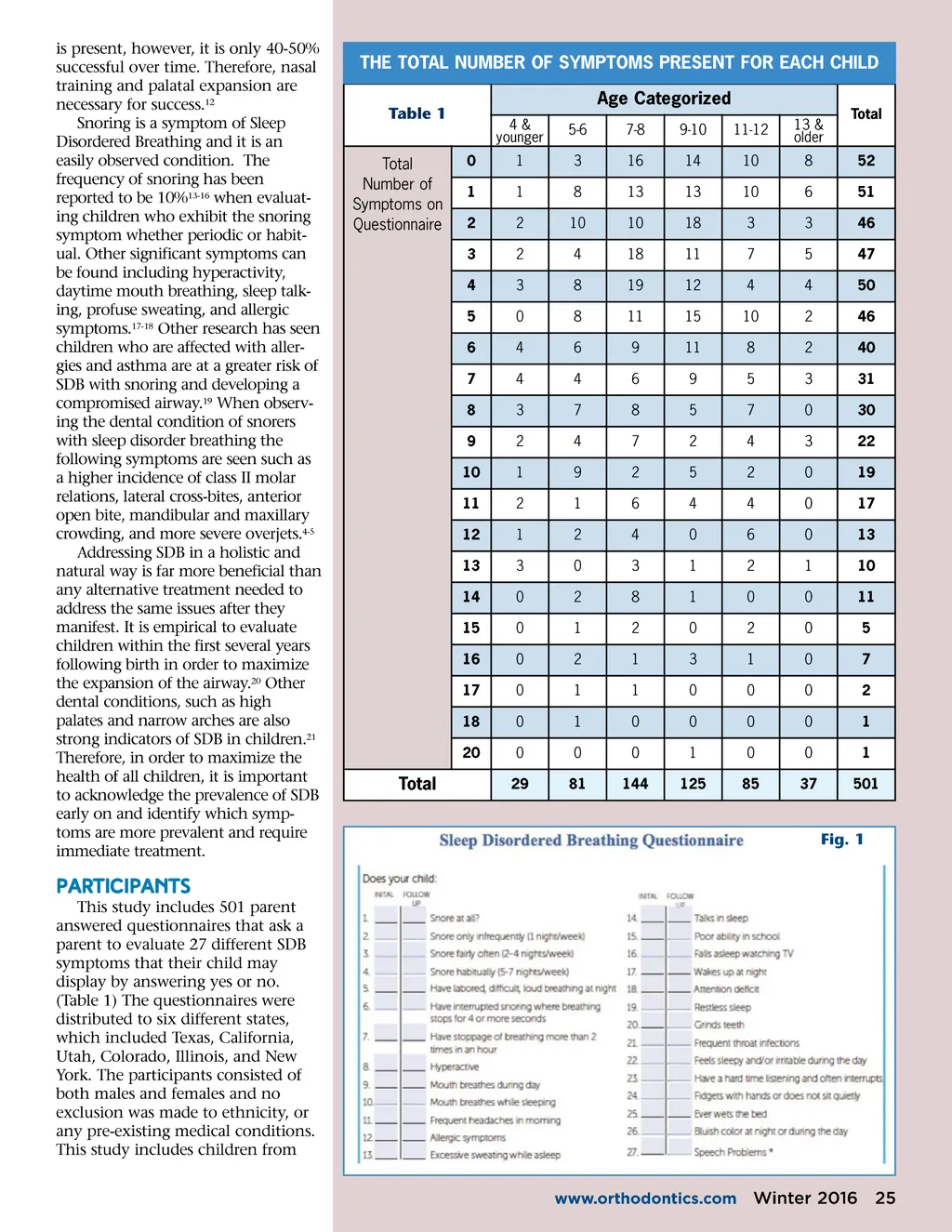
By Brooke Stevens, BS, University of Michigan and Earl O. Bergersen, DDS, MSD leep Disordered Breathing (SDB) has been found to be a root cause for many child-hood health and behavioral conditions. This study consisting of 501 children ages from 2 to 19 years of age assess SDB in children through a parent questionnaire containing 27 items, which reflect various health and behavioral issues in children. This study found that 9 out of 10 children display at least one symp-tom of SDB. Prevalent symptoms include snoring, mouth breathing, talking in sleep, difficulty listening, teeth grinding, and bed-wetting. It is important to address these health issues early on in order to allow chil-dren to thrive and enjoy a long healthy life with a normal airway. S Review of Literature Sleep Disordered Breathing (SDB) is a condition that results from a compromised airway causing irregu-larities in the gas exchange, home-ostasis, and restorative processes occurring during sleep. 1 SDB is asso-ciated with an expansive range of clinical symptoms, environmental and genetic factors, and dentofacial physical examination findings. 2 Some of these common clinical symptoms include mouth breathing, snoring, teeth grinding, bed-wetting, ADD/ADHD, and many more. Impli-cations of improper breathing can be detrimental if not addressed as reduced oxygenation can negatively impact a child’s ability to succeed in school and day-to-day life. 3 Two of the most frequent symp-toms involving sleep disordered breathing include daytime and nighttime open-mouth breathing 4 and habitual snoring. 5 It is important that SDB breathing symptoms are recognized and addressed early on. The symptom of mouth breathing is considered a very critical symptom when evaluating a child for Sleep Disordered Breathing which was seen in an experiment conducted on Rhesus monkeys by obstructing the nasal cavity, thereby producing mouth breathing which resulted in a narrowing of dental arches, decreased maxillary arch length, tongue function, increased anterior facial height, anterior cross-bite, and maxillary overjet. 6-8 Other conditions resulting from mouth breathing in children can be directly related to enlarged tonsils resulting in a tongue thrust. These enlarged tonsils displace the tongue in the mouth promoting a tongue thrust and mouth breathing. 9-10 Mouth breathing can involve a combination of frequent throat infections, abnor-mal development of a malocclusion, improper phonation, and changes in sleep. 11 Further complications can occur and should be addressed in the evaluation of the tonsils. A Tonsillec-tomy and adenoidectomy are often recommended at an early age if SDB 24 Winter 2016 JAOS
Journal of the American Orthodontic Society Winter 2016: Page 24